JACC: Cardiovascular Imaging ( IF 12.8 ) Pub Date : 2021-12-15 , DOI: 10.1016/j.jcmg.2021.10.017 Miguel Cainzos-Achirica 1 , Renato Quispe 2 , Ramzi Dudum 3 , Philip Greenland 4 , Donald Lloyd-Jones 4 , Jamal S Rana 5 , Joao A C Lima 6 , Henrique Doria de Vasconcellos 6 , Parag H Joshi 7 , Amit Khera 7 , Colby Ayers 7 , Raimund Erbel 8 , Andreas Stang 9 , Karl-Heinz Jöckel 8 , Nils Lehmann 8 , Sara Schramm 8 , Börge Schmidt 8 , Peter P Toth 10 , Kershaw V Patel 11 , Michael J Blaha 12 , Marcio Bittencourt 13 , Khurram Nasir 1
|
Objectives
In this study, we sought to evaluate whether the coronary artery calcium (CAC) score can enhance current paradigms for risk stratification among individuals with hypertriglyceridemia in primary prevention. The eligibility criteria for icosapent ethyl (IPE) were used as case example.
Background
Recent trials of atherosclerotic cardiovascular disease (ASCVD) risk-reduction therapies for individuals with hypertriglyceridemia without clinical ASCVD restricted enrollment to participants with diabetes or various other risk factors. These criteria were mirrored in the Food and Drug Administration product label for IPE.
Methods
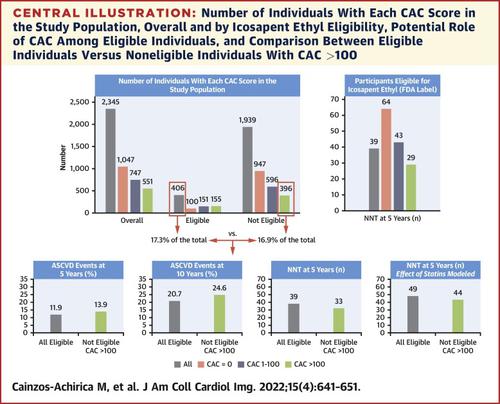
We pooled 2,345 participants with triglycerides 150 to <500 mg/dL (or >178-<500 mg/dL if not on a statin) and without clinical ASCVD from MESA, CARDIA, the Dallas Heart Study, and the Heinz Nixdorf Recall study. We evaluated the incidence of ASCVD events overall, by IPE eligibility (as defined in the product label), and further stratified by CAC scores (0, >0-100, >100). The number needed to treat for 5 years (NNT5) to prevent 1 event was estimated among IPE-eligible participants, assuming a 21.8% relative risk reduction with IPE. In exploratory analyses, the NNT5 was also estimated among noneligible participants.
Results
There was marked heterogeneity in CAC burden overall (45% CAC 0; 24% CAC >100) and across IPE eligibility strata. Overall, 17% of participants were eligible for IPE and 11.9% had ASCVD events within 5 years. Among participants eligible for IPE, 38% had CAC >100, and their event rates were markedly higher (15.9% vs 7.2%) and the NNT5 2.2-fold lower (29 vs 64) than those of the 25% eligible participants with CAC 0. Among the 83% participants not eligible for IPE, 20% had CAC >100, and their 5-year incidence of ASCVD (13.9%) was higher than the overall incidence among IPE-eligible participants.
Conclusions
CAC can improve current risk stratification and therapy allocation paradigms among individuals with hypertriglyceridemia without clinical ASCVD. Future trials of risk-reduction therapies in hypertriglyceridemia could use CAC >100 to enroll a high-risk study sample, with implications for a larger target population.
中文翻译:
CAC 用于无临床动脉粥样硬化性心血管疾病的高甘油三酯血症个体的风险分层
目标
在这项研究中,我们试图评估冠状动脉钙化 (CAC) 评分是否可以增强目前在一级预防中高甘油三酯血症患者的风险分层范式。以二十碳五烯酸乙酯 (IPE) 的资格标准为例。
背景
最近对没有临床 ASCVD 的高甘油三酯血症患者进行的动脉粥样硬化性心血管疾病 (ASCVD) 风险降低治疗试验限制了患有糖尿病或其他各种风险因素的参与者的招募。这些标准反映在食品和药物管理局的 IPE 产品标签中。
方法
我们汇集了来自 MESA、CARDIA、达拉斯心脏研究和 Heinz Nixdorf 召回研究的 2,345 名甘油三酯 150 至 <500 mg/dL(或 >178-<500 mg/dL,如果未服用他汀类药物)且无临床 ASCVD 的参与者。我们通过 IPE 资格(如产品标签中定义)评估了总体 ASCVD 事件的发生率,并通过 CAC 评分(0、>0-100、>100)进一步分层。在符合 IPE 条件的参与者中估计需要治疗 5 年 (NNT 5 ) 以预防 1 次事件的人数,假设 IPE 的相对风险降低 21.8%。在探索性分析中,NNT 5也在不合格参与者中进行了估计。
结果
总体 CAC 负担(45% CAC 0;24% CAC >100)和跨 IPE 资格层级存在显着异质性。总体而言,17% 的参与者符合 IPE 条件,11.9% 的参与者在 5 年内发生 ASCVD 事件。在符合 IPE 条件的参与者中,38% 的 CAC > 100,与 25% 符合条件的 CAC 参与者相比,他们的事件发生率显着更高(15.9% 比 7.2%)和 NNT 5低 2.2 倍(29 比 64) 0. 83%不符合IPE条件的参与者中,20%的CAC>100,其5年ASCVD发病率(13.9%)高于IPE合格参与者的总体发病率。
结论
CAC 可以改善目前没有临床 ASCVD 的高甘油三酯血症患者的风险分层和治疗分配模式。未来对高甘油三酯血症风险降低疗法的试验可以使用 CAC > 100 来招募高风险研究样本,这对更大的目标人群有影响。










































 京公网安备 11010802027423号
京公网安备 11010802027423号