JACC: Cardiovascular Imaging ( IF 12.8 ) Pub Date : 2021-12-15 , DOI: 10.1016/j.jcmg.2021.10.015 Tom Kai Ming Wang 1 , Kevser Akyuz 1 , Amgad Mentias 1 , Jason Kirincich 1 , Alejandro Duran Crane 1 , Samantha Xu 1 , Zoran B Popovic 1 , Bo Xu 1 , A Marc Gillinov 2 , Gosta B Pettersson 2 , Brian P Griffin 1 , Milind Y Desai 1
|
Objectives
The authors report etiologies and outcomes and devise a risk model in a large contemporary cohort of patients with isolated tricuspid regurgitation (TR).
Background
Isolated TR is a challenging clinical entity with heterogeneous etiology and often poor outcomes, with a paucity of recent research regarding the epidemiology of isolated TR.
Methods
Consecutive patients with isolated TR graded at least moderate to severe on echocardiography from January 2004 to December 2018 (n = 9,045, mean age 70.4 ± 15.4 years, 60.3% women) were studied. TR etiologies were individually adjudicated as secondary or primary, with subcategories. All-cause death during follow-up was the primary endpoint, with associations between etiology and outcomes analyzed and a risk model created.
Results
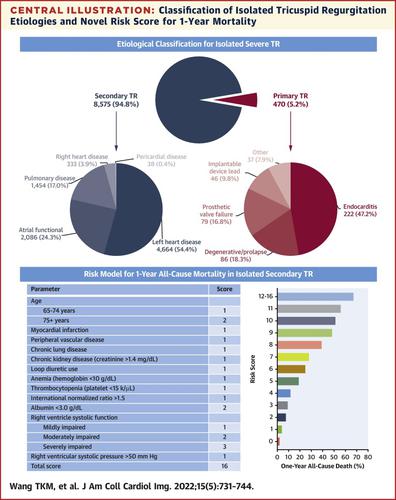
Primary and secondary TR etiologies were present in 470 (5.2%) and 8,575 (94.8%) patients, respectively. The main secondary etiologies were left heart disease in 4,664 (54.4%), atrial functional in 2,086 (24.3%), and pulmonary disease in 1,454 (17.0%), and the main primary etiologies were endocarditis in 222 (47.2%), degenerative or prolapse in 86 (18.3%), and prosthetic valve failure in 79 (16.8%). There were 3,987 deaths (44.0%) over a mean follow-up period of 2.6 ± 3.3 years. In unadjusted analyses, patients with secondary TR had worse survival than those with primary TR (HR: 1.56; 95% CI: 1.32-1.85), but this result was not statistically significant in multivariable analysis. The authors devised and internally validated a risk score for predicting 1-year mortality in these patients.
Conclusions
Secondary TR constituted 95% of isolated significant TR and conferred worse survival than primary TR in unadjusted but not adjusted analyses. The present novel risk score stratifies the risk for 1-year death and may influence decision making for management in these high-risk patients.
中文翻译:
孤立性三尖瓣关闭不全的当代病因、结果和新的风险评分
目标
作者报告了病因和结果,并在当代大型孤立性三尖瓣反流 (TR) 患者队列中设计了风险模型。
背景
孤立性 TR 是一个具有挑战性的临床实体,具有异质的病因和通常较差的结果,最近关于孤立性 TR 流行病学的研究很少。
方法
研究了 2004 年 1 月至 2018 年 12 月超声心动图分级至少为中度至重度的连续孤立性 TR 患者(n = 9,045,平均年龄 70.4 ± 15.4 岁,60.3% 的女性)。TR 病因被单独裁定为继发性或原发性,并具有子类别。随访期间的全因死亡是主要终点,分析了病因和结果之间的关联并创建了风险模型。
结果
原发性和继发性 TR 病因分别存在于 470 名 (5.2%) 和 8,575 名 (94.8%) 患者中。主要继发性病因是左心病 4,664 人(54.4%),心房功能障碍 2,086 人(24.3%),肺部疾病 1,454 人(17.0%),主要原发性病因是心内膜炎 222 人(47.2%)、退行性或86 人(18.3%)脱垂,79 人(16.8%)人工瓣膜失败。在 2.6 ± 3.3 年的平均随访期内,有 3,987 人死亡(44.0%)。在未经调整的分析中,继发性 TR 患者的生存率低于原发性 TR 患者(HR:1.56;95% CI:1.32-1.85),但这一结果在多变量分析中无统计学意义。作者设计并内部验证了用于预测这些患者 1 年死亡率的风险评分。
结论
在未调整但未调整的分析中,次要 TR 占孤立显着 TR 的 95%,并且比主要 TR 的生存率更差。目前的新风险评分对 1 年死亡风险进行了分层,并可能影响这些高风险患者的管理决策。










































 京公网安备 11010802027423号
京公网安备 11010802027423号