JACC: Cardiovascular Imaging ( IF 12.8 ) Pub Date : 2021-11-17 , DOI: 10.1016/j.jcmg.2021.09.013 Robin F Gohmann 1 , Konrad Pawelka 1 , Patrick Seitz 2 , Nicolas Majunke 3 , Linda Heiser 2 , Katharina Renatus 1 , Steffen Desch 3 , Philipp Lauten 3 , David Holzhey 4 , Thilo Noack 4 , Johannes Wilde 3 , Philipp Kiefer 4 , Christian Krieghoff 2 , Christian Lücke 2 , Sebastian Gottschling 2 , Sebastian Ebel 1 , Michael A Borger 5 , Holger Thiele 6 , Christoph Panknin 7 , Matthias Horn 8 , Mohamed Abdel-Wahab 3 , Matthias Gutberlet 9
|
Objectives
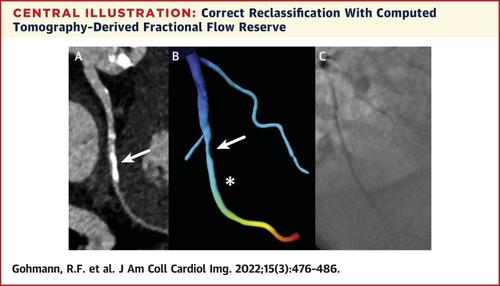
The purpose of this study was to analyze the ability of machine-learning (ML)-based computed tomography (CT)-derived fractional flow reserve (CT-FFR) to further improve the diagnostic performance of coronary CT angiography (cCTA) for ruling out significant coronary artery disease (CAD) during pre-transcatheter aortic valve replacement (TAVR) evaluation in patients with a high pre-test probability for CAD.
Background
CAD is a frequent comorbidity in patients undergoing TAVR. Current guidelines recommend its assessment before TAVR. If significant CAD can be excluded on cCTA, invasive coronary angiography (ICA) may be avoided. Although cCTA is a very sensitive test, it is limited by relatively low specificity and positive predictive value, particularly in high-risk patients.
Methods
Overall, 460 patients (age 79.6 ± 7.4 years) undergoing pre-TAVR CT were included and examined with an electrocardiogram-gated CT scan of the heart and high-pitch scan of the vascular access route. Images were evaluated for significant CAD. Patients routinely underwent ICA (388/460), which was omitted at the discretion of the local Heart Team if CAD could be effectively ruled out on cCTA (72/460). CT examinations in which CAD could not be ruled out (CAD+) (n = 272) underwent additional ML-based CT-FFR.
Results
ML-based CT-FFR was successfully performed in 79.4% (216/272) of all CAD+ patients and correctly reclassified 17 patients as CAD negative. CT-FFR was not feasible in 20.6% because of reduced image quality (37/56) or anatomic variants (19/56). Sensitivity, specificity, positive predictive value, and negative predictive value were 94.9%, 52.0%, 52.2%, and 94.9%, respectively. The additional evaluation with ML-based CT-FFR increased accuracy by Δ+3.4% (CAD+: Δ+6.0%) and raised the total number of examinations negative for CAD to 43.9% (202/460).
Conclusions
ML-based CT-FFR may further improve the diagnostic performance of cCTA by correctly reclassifying a considerable proportion of patients with morphological signs of obstructive CAD on cCTA during pre-TAVR evaluation. Thereby, CT-FFR has the potential to further reduce the need for ICA in this challenging elderly group of patients before TAVR.
中文翻译:
结合 cCTA 和 TAVR 计划以排除重大 CAD
目标
本研究的目的是分析基于机器学习 (ML) 的计算机断层扫描 (CT) 衍生的血流储备分数 (CT-FFR) 的能力,以进一步提高冠状动脉 CT 血管造影 (cCTA) 的诊断性能以排除在经导管主动脉瓣置换术 (TAVR) 评估期间对具有高 CAD 预测试概率的患者进行显着冠状动脉疾病 (CAD)。
背景
CAD 是接受 TAVR 的患者的常见合并症。当前指南建议在 TAVR 之前对其进行评估。如果 cCTA 可以排除严重的 CAD,则可以避免侵入性冠状动脉造影 (ICA)。尽管 cCTA 是一种非常敏感的测试,但它受限于相对较低的特异性和阳性预测值,尤其是在高危患者中。
方法
总体而言,纳入了 460 名接受 TAVR 前 CT 的患者(年龄 79.6 ± 7.4 岁),并通过心脏的心电图门控 CT 扫描和血管通路的高螺距扫描进行了检查。对图像进行了显着 CAD 评估。患者常规接受 ICA (388/460),如果 cCTA 可以有效排除 CAD (72/460),则由当地心脏团队酌情省略。不能排除 CAD 的 CT 检查 (CAD + ) (n = 272) 接受了额外的基于 ML 的 CT-FFR。
结果
在所有 CAD +患者中,79.4% (216/272) 成功执行了基于 ML 的 CT-FFR,并将 17 名患者正确重新分类为 CAD 阴性。由于图像质量下降 (37/56) 或解剖变异 (19/56),CT-FFR 在 20.6% 中不可行。敏感性、特异性、阳性预测值和阴性预测值分别为94.9%、52.0%、52.2%和94.9%。使用基于 ML 的 CT-FFR 进行的额外评估将准确度提高了 Δ+3.4%(CAD +:Δ+6.0%),并将 CAD 阴性的检查总数提高到 43.9% (202/460)。
结论
基于 ML 的 CT-FFR 可以通过在 TAVR 前评估期间正确重新分类相当一部分在 cCTA 上具有阻塞性 CAD 形态学迹象的患者,从而进一步提高 cCTA 的诊断性能。因此,在 TAVR 之前,CT-FFR 有可能进一步减少这一具有挑战性的老年患者群体对 ICA 的需求。










































 京公网安备 11010802027423号
京公网安备 11010802027423号