International Journal of Cardiology ( IF 3.2 ) Pub Date : 2021-10-30 , DOI: 10.1016/j.ijcard.2021.10.149 Jan Biegus 1 , Sylwia Nawrocka-Millward 2 , Robert Zymliński 1 , Marat Fudim 3 , Jeffrey Testani 4 , Dominik Marciniak 5 , Marta Rosiek-Biegus 6 , Barbara Ponikowska 7 , Mateusz Guzik 2 , Mateusz Garus 2 , Piotr Ponikowski 1
|
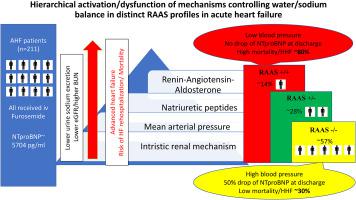
Background: Although renin-angiotensin-aldosterone system (RAAS) activation is believed to be the major driver of acute heart failure (AHF) episodes our understanding of its prevalence and clinical relevance in contemporary settings is incomplete. Methods: Serum renin and aldosterone were measured at day-1 and at discharge in patients (n = 211) that were hospitalized between 2016 and 2017 for AHF in a single cardiology center. The population was profiled based on upper limits of normal (ULN) of both biomarkers assessed at day-1 and linked with the clinical course and outcomes. Results: The study population constituted of three profiles: RAAS−/− (n = 121 [57%]); RAAS+/− (n = 60 [28%]); and RAAS+/+ (n = 30 [14%]). The RAAS+/+ profile had the lowest blood pressure and serum sodium at admission, day-2 and discharge compared to the other profiles (p < 0.001). The RAAS+/+ patients had significantly lower urine Na+ at admission (57.8 ± 36.7 vs 97.3 ± 31.3 and 86.4 ± 35.0), day-1 (52.7 ± 32.7 vs 85.3 ± 36.3 and 75.5 ± 33.9) mmol/l, vs RAAS−/− and RAAS+/− profiles, respectively, all p < 0.001. There was also a gradual decrease of renal function across increasing RAAS profiles. The RAAS+/+ profile received higher dose of furosemide at discharge 120 [80–160] vs the other profiles 80 [40–120] mg, p < 0.01. The risks of one year mortality or HF rehospitalization increased across the RAAS profiles (p < 0.001). The trajectory of renin or aldosterone change during hospitalization was not related to outcomes. Conclusions: The RAAS overactivity is not essential for development of AHF. However, elevated RAAS is a marker of more advanced stages of heart failure, is related to low natriuresis and adverse clinical outcomes.
中文翻译:
不同的肾素/醛固酮活性谱与肾功能、利尿钠反应、去充血能力和急性心力衰竭预后相关
背景:虽然肾素-血管紧张素-醛固酮系统 (RAAS) 激活被认为是急性心力衰竭 (AHF) 发作的主要驱动因素,但我们对其在当代环境中的患病率和临床相关性的理解尚不完整。 方法:在 2016 年至 2017 年期间在单个心脏病中心住院的 AHF患者( n = 211)在第 1 天和出院时测量血清肾素和醛固酮。根据第 1 天评估的两种生物标志物的正常上限 (ULN) 对人群进行分析,并与临床过程和结果相关联。结果:研究人群由三个概况组成:RAAS-/-(n = 121 [57%]);RAAS+/- ( n = 60 [28%]); 和 RAAS+/+ ( n = 30 [14%])。与其他曲线相比,RAAS+/+ 曲线在入院、第 2 天和出院时具有最低的血压和血清钠(p < 0.001)。RAAS+/+ 患者入院时尿 Na+ 显着降低(57.8 ± 36.7 vs 97.3 ± 31.3 和 86.4 ± 35.0),第 1 天(52.7 ± 32.7 vs 85.3 ± 36.3 和 75.5 ± 33.9)mmol/l, vs RAAS-/ − 和 RAAS+/- 曲线分别为p < 0.001。随着 RAAS 谱的增加,肾功能也逐渐下降。RAAS+/+ 曲线在出院时接受了更高剂量的呋塞米 120 [80-160],而其他曲线为 80 [40-120] mg,p < 0.01。一年死亡率或心衰再住院的风险在 RAAS 概况中有所增加(p < 0.001)。住院期间肾素或醛固酮变化的轨迹与结局无关。结论:RAAS 过度活跃对于 AHF 的发展不是必需的。然而,升高的 RAAS 是心力衰竭更晚期的标志,与低尿钠排泄和不良临床结果有关。










































 京公网安备 11010802027423号
京公网安备 11010802027423号