Heart Rhythm ( IF 5.5 ) Pub Date : 2021-10-30 , DOI: 10.1016/j.hrthm.2021.10.025 Pablo Salazar 1 , Andrew D Beaser 1 , Gaurav A Upadhyay 1 , Zaid Aziz 1 , Stephanie Besser 1 , Dalise Y Shatz 1 , Hemal M Nayak 1 , Roderick Tung 1
|
Background
Catheter ablation strategies for ventricular fibrillation (VF) and polymorphic ventricular tachycardia (PMVT) are not established when spontaneous triggers are rare or absent.
Objective
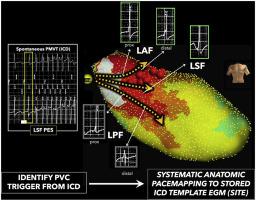
The purpose of this study was to report the feasibility and efficacy of a novel empiric ablation strategy of pacemapping to stored implantable cardioverter-defibrillator (ICD) template electrograms (SITE) of the clinical premature ventricular contraction (PVC) trigger.
Methods
Fifteen patients with drug-refractory VF/PMVT receiving defibrillator shocks without identifiable and mappable PVC triggers were prospectively analyzed. The protocol incorporated systematic pacemapping from known arrhythmogenic sites (moderator band/right ventricular [RV] papillary muscles, left conduction system/Purkinje network, outflow tracts) with real-time comparison between the paced ICD electrogram (EGM) morphology and SITE.
Results
Regions within the left Purkinje network yielded the best pacemap match for the SITE of the clinical PVC trigger in 55% of ablation targets (left posterior fascicle 6, left septal fascicle 1, left anterior fascicle 5), followed by the RV moderator band region in 14% (n = 3), RV papillary muscles in 13% (n = 3), periaortic region in 14% (n = 3), and left ventricular anterolateral papillary muscle in 4% (n = 1). Freedom from ICD therapies off antiarrhythmic drug (AAD) was 64% at 6 months and 48% at 12 months. Shock burden was reduced from 4 (2–6) to 0 (0–1) (P = .001), and use of AADs was reduced from 2 (1–2) to 0 (0–1) (P = .001).
Conclusion
In the absence of a mappable trigger, an empiric strategy of interrogating the Purkinje network, papillary muscles, and outflow tract regions by pacemap matching with SITE of the clinical PVC is feasible to guide ablation. A significant reduction in VF/PMVT therapy burden and AAD utilization was observed after a single procedure.
中文翻译:
在没有可映射触发器的情况下经验性消融多形性室性心动过速/纤颤:起搏图与除颤器电图匹配的前瞻性可行性和有效性
背景
当自发性触发因素很少或不存在时,心室颤动 (VF) 和多形性室性心动过速 (PMVT) 的导管消融策略尚未确定。
客观的
本研究的目的是报告一种新的起搏经验消融策略对临床室性早搏 (PVC) 触发器的存储的植入式心脏复律除颤器 (ICD) 模板电图 (SITE) 的可行性和有效性。
方法
前瞻性分析了 15 名药物难治性 VF/PMVT 患者接受除颤器电击而没有可识别和可映射的 PVC 触发器。该协议结合了来自已知致心律失常部位(调节带/右心室 [RV] 乳头肌、左传导系统/浦肯野网络、流出道)的系统起搏映射,并在起搏 ICD 电图 (EGM) 形态和 SITE 之间进行了实时比较。
结果
左侧浦肯野网络内的区域在 55% 的消融目标(左后束 6、左间隔束 1、左前束 5)中与临床 PVC 触发的 SITE 产生了最佳的起搏图匹配,其次是 RV 调节带区域14% (n = 3),RV 乳头肌 13% (n = 3),主动脉周围区 14% (n = 3),左心室前外侧乳头肌 4% (n = 1)。在第 6 个月和第 12 个月时,免于 ICD 治疗的抗心律失常药物 (AAD) 为 64% 和 48%。休克负担从 4 (2-6) 减少到 0 (0-1) ( P = .001),AAD 的使用从 2 (1-2) 减少到 0 (0-1) ( P = .001 )。
结论
在没有可映射触发器的情况下,通过与临床 PVC 的 SITE 匹配的起搏图来询问浦肯野网络、乳头肌和流出道区域的经验策略是可行的,以指导消融。单次手术后观察到 VF/PMVT 治疗负担和 AAD 利用率显着降低。


























 京公网安备 11010802027423号
京公网安备 11010802027423号