Heart Rhythm ( IF 5.6 ) Pub Date : 2021-09-30 , DOI: 10.1016/j.hrthm.2021.09.028 Martín R Arceluz 1 , Ioan Liuba 1 , Cory M Tschabrunn 1 , David S Frankel 1 , Pasquale Santangeli 1 , Gregory E Supple 1 , Robert D Schaller 1 , Fermin C Garcia 1 , David J Callans 1 , Gustavo S Guandalini 1 , Katie Walsh 1 , Saman Nazarian 1 , Erica S Zado 1 , Francis E Marchlinski 1
|
Background
Ventricular tachycardia (VT) substrate in left ventricular (LV) nonischemic cardiomyopathy (NICM) consists of fibrosis with surviving myocardium.
Objective
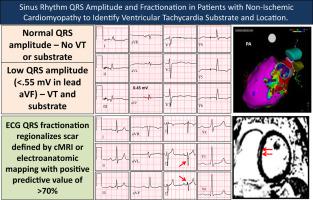
The purpose of this study was to determine whether, in patients with LV NICM and sustained VT, reduced QRS amplitude and QRSf during sinus rhythm can identify the presence and location of abnormal septal (S-NICM) and/or free-wall (FW-NICM) VT substrate.
Methods
We compared patients with NICM and VT (group 1) with electroanatomic mapping septal (S-NICM; n = 21) or free-wall (FW-NICM; n = 20) VT substrate to a 38-patient reference cohort (group 2) with cardiac magnetic resonance imaging (cMRI) and NICM but no VT referred for primary prevention implantable cardioverter-defibrillator (26 [68.4%] with late gadolinium enhancement).
Results
Group 1 had lower QRS amplitude in leads II (0.60 ± 0.22 vs 0.86 ± 0.35, P <.001), aVR (0.60 ± 0.24 vs 0.75 ± 0.31, P = .002), aVF (0.48 ± 0.20 vs 0.70 ± 0.28, P <.001), and V2 (1.09 ± 0.52 vs 1.38 ± 0.55, P = .001) than group 2. QRS <0.55 mV in lead aVF identified VT and accompanying substrate with sensitivity 70% and specificity 71%. Most group 1 and group 2 patients had 12-lead ECG QRS fractionation (QRSf) in ≥2 contiguous leads (78% vs 63.2%, P = .14). Sensitivity and specificity for ≥2 QRSf leads identifying respective regional electroanatomic or cMRI abnormalities were 76% and 50% for inferior, 44% and 87% for lateral, and 21% and 89% for anterior leads.
Conclusion
In LV NICM, low frontal plane QRS (<0.55 mV in aVF) is associated with VT substrate. Although multilead QRS fractionation is associated with the presence and location of VT substrate, it is frequently identified in patients without VT with cMRI abnormalities.
中文翻译:
非缺血性心肌病患者的窦性心律 QRS 波幅和分割以识别室性心动过速的底物和位置
背景
左心室 (LV) 非缺血性心肌病 (NICM) 中的室性心动过速 (VT) 基质由存活心肌的纤维化组成。
客观的
本研究的目的是确定在 LV NICM 和持续 VT 患者中,窦性心律期间 QRS 波幅和 QRSf 降低是否可以识别异常间隔 (S-NICM) 和/或游离壁 (FW- NICM) VT 底物。
方法
我们将 NICM 和 VT 患者(第 1 组)与电解剖标测间隔(S-NICM;n = 21)或游离壁(FW-NICM;n = 20)VT 底物与 38 名患者参考队列(第 2 组)心脏磁共振成像 (cMRI) 和 NICM,但没有 VT 转诊为一级预防植入式心脏复律除颤器(26 [68.4%] 晚期钆增强)。
结果
第 1 组在 II 导联 (0.60 ± 0.22 vs 0.86 ± 0.35, P <.001)、aVR (0.60 ± 0.24 vs 0.75 ± 0.31, P = .002)、aVF (0.48 ± 0.20 vs 0.70 ± 0.28, P <.001) 和 V 2 (1.09 ± 0.52 vs 1.38 ± 0.55, P = .001) 比第 2 组。aVF 导联中的 QRS <0.55 mV 可识别 VT 和伴随基质,灵敏度为 70%,特异性为 71%。大多数第 1 组和第 2 组患者在≥2 个连续导联中具有 12 导联心电图 QRS 分割 (QRSf)(78% 对 63.2%,P = .14)。识别相应区域电解剖或 cMRI 异常的≥2 个 QRSf 导联的敏感性和特异性分别为:下位导联为 76% 和 50%,侧导联为 44% 和 87%,前路导联为 21% 和 89%。
结论
在 LV NICM 中,低额平面 QRS(aVF 中 <0.55 mV)与 VT 底物相关。虽然多导联 QRS 分割与 VT 基底的存在和位置有关,但它经常在没有 VT 且 cMRI 异常的患者中被发现。








































 京公网安备 11010802027423号
京公网安备 11010802027423号