Kidney International ( IF 14.8 ) Pub Date : 2021-09-22 , DOI: 10.1016/j.kint.2021.08.025 Kavita Gulati 1 , Helena Edwards 2 , Maria Prendecki 1 , Thomas D Cairns 2 , Marie Condon 2 , Jack Galliford 2 , Megan Griffith 1 , Jeremy B Levy 1 , Frederick W K Tam 1 , Anisha Tanna 2 , Charles D Pusey 1 , Stephen P McAdoo 1
|
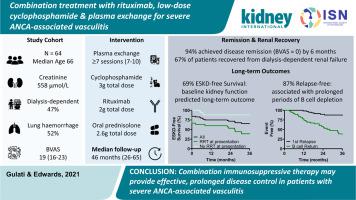
Antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis can present with life-threatening lung-kidney syndromes. However, many controlled treatment trials excluded patients with diffuse alveolar hemorrhage or severely impaired glomerular filtration rates, and so the optimum treatment in these cases is unclear. In this retrospective cohort study, we report the outcomes of 64 patients with life-threatening disease treated with a combination regimen of rituximab, low-dose intravenous cyclophosphamide, oral glucocorticoids, and plasma exchange. At entry, the median estimated glomerular filtration rate was 9 mL/min, 47% of patients required dialysis, and 52% had diffuse alveolar hemorrhage. All patients received a minimum of seven plasma exchanges, and the median cumulative doses of rituximab, cyclophosphamide, and glucocorticoid were 2, 3, and 2.6 g, respectively, at six months. A total of 94% of patients had achieved disease remission (version 3 Birmingham Vasculitis Activity Score of 0) at this time point, and 67% of patients who required dialysis recovered independent kidney function. During long-term follow-up (median duration 46 months), overall patient survival was 85%, and 69% of patients remained free from end-stage kidney disease, which compares favorably to a historic cohort with severe disease treated with a conventional induction regimen. Combination treatment was associated with prolonged B cell depletion and low rates of relapse; 87% of patients were in continuous remission at month 36. The serious infection rate during total follow-up was 0.28 infections/patient/year, suggesting that combination treatment is not associated with an enduring risk of infection. Thus, we suggest that combination immunosuppressive therapy may permit glucocorticoid avoidance and provide rapid and prolonged disease control in patients with severe ANCA-associated vasculitis.
中文翻译:
联合利妥昔单抗、低剂量环磷酰胺和血浆置换治疗严重抗中性粒细胞胞浆抗体相关性血管炎
抗中性粒细胞胞浆抗体 (ANCA) 相关性血管炎可出现危及生命的肺肾综合征。然而,许多对照治疗试验排除了弥漫性肺泡出血或肾小球滤过率严重受损的患者,因此这些病例的最佳治疗尚不清楚。在这项回顾性队列研究中,我们报告了 64 名危及生命疾病患者接受利妥昔单抗、低剂量静脉环磷酰胺、口服糖皮质激素和血浆置换联合治疗的结果。入组时,估计肾小球滤过率中位数为 9 mL/min,47% 的患者需要透析,52% 的患者有弥漫性肺泡出血。所有患者至少接受了 7 次血浆置换,利妥昔单抗、环磷酰胺和糖皮质激素的中位累积剂量分别为 2、3、和 2.6 克,分别在六个月。在这个时间点,共有 94% 的患者实现了疾病缓解(第 3 版伯明翰血管炎活动评分为 0),67% 的需要透析的患者恢复了独立的肾功能。在长期随访期间(中位时间为 46 个月),患者的总生存率为 85%,69% 的患者未患终末期肾病,这与接受传统诱导治疗的严重疾病的历史队列相比是有利的养生法。联合治疗与延长 B 细胞耗竭和低复发率有关;87% 的患者在第 36 个月持续缓解。总随访期间的严重感染率为 0.28 感染/患者/年,这表明联合治疗与持久感染风险无关。因此,










































 京公网安备 11010802027423号
京公网安备 11010802027423号