Pediatric Nephrology ( IF 2.6 ) Pub Date : 2021-09-21 , DOI: 10.1007/s00467-021-05197-3 Rohit Bhowmick 1 , Ramachandran Rameshkumar 1 , Madhusudhanan Ponnusamy 2 , Vishnukumar Rajaraman 2 , Muthu Chidambaram 1, 3 , Abraar Sheriff 1 , Subramanian Mahadevan 1
|
Background
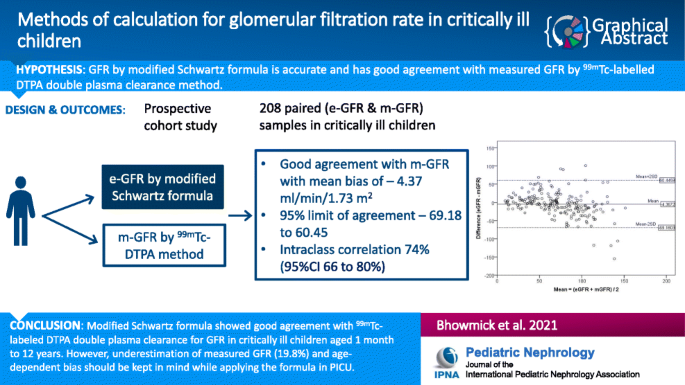
Studies comparing the modified Schwartz formula with measured GFR (m-GFR) are lacking in critically ill children.
Methods
This prospective cohort study enrolled children aged 1 month to 12 years, within 24 h of admission. m-GFR measured by technetium-99m-labeled diethylenetriaminepentaacetic acid (99mTc-DTPA) and calculated by Russell’s two-sample slope-intercept method. Serum creatinine was estimated by modified Jaffe method and estimated GFR (e-GFR) calculated by modified Schwartz formula. The primary outcome was to find agreement between the two methods. Bias, precision, and accuracy were calculated. Secondary outcomes were the incidence of AKI (by p-RIFLE criteria) and the difference between the two methods to diagnose AKI.
Results
A total of 208 pairs were analyzed. e-GFR showed good agreement with m-GFR with a mean bias of –4.37 ml/min/1.73 m2 and precision (SD of bias) of 33.07, 95% limit of agreement –69.18 to 60.45, and intraclass correlation of 74% (95%CI 66–80%, P < 0.001). e-GFR underestimated m-GFR by 19.8% (95% CI 7.9–31.7%). Accuracy of e-GFR values within 10%, 20%, and 30% of m-GFR were 68.3%, 72.6%, and 78.8%, respectively. Incidence of AKI within 24 h was 60.1% by e-GFR and 54.3% by m-GFR (kappa 0.569, P < 0.001; sensitivity of 85.8%, 95%CI (78–91.7%).
Conclusions
The modified Schwartz formula shows good agreement with 99mTc-labeled DTPA double plasma sample clearance method for calculating GFR in critically ill children aged 1 month to 12 years. The underestimation of GFR should be kept in mind while applying the formula at the bedside in PICU.
Trial registration
Protocol accessible at Clinical Trial Registry of India (CTRI) www.ctri.nic.in. (Trial Registered Prospectively and Registration No. CTRI/2017/10/010014) ([Registered on: 06/10/2017] Trial Registered Prospectively.) (Title “Measured glomerular filtration rate using Diethylenetriaminepentaacetic acid (DTPA) renal scan versus estimated glomerular filtration rate using modified Schwartz formula in critically ill children: A prospective observational, analytical study.”).
Graphical abstract
中文翻译:
修正 Schwartz 公式和 99mTc-DTPA 血浆清除率计算危重患儿肾小球滤过率
背景
在危重儿童中缺乏将改良 Schwartz 公式与测量的 GFR (m-GFR) 进行比较的研究。
方法
这项前瞻性队列研究在入院后 24 小时内招募了 1 个月至 12 岁的儿童。m-GFR 通过锝 99m 标记的二亚乙基三胺五乙酸 ( 99m Tc-DTPA) 测量并通过 Russell 的双样本斜率截距法计算。血清肌酐采用改良的 Jaffe 法估算,估算的 GFR(e-GFR)采用改良的 Schwartz 公式计算。主要结果是找到两种方法之间的一致性。计算偏差、精度和准确度。次要结果是 AKI 的发生率(根据 p-RIFLE 标准)以及两种诊断 AKI 方法之间的差异。
结果
共分析了 208 对。e-GFR 与 m-GFR 具有良好的一致性,平均偏差为 –4.37 ml/min/1.73 m 2,精度(偏差的 SD)为 33.07,95% 的一致性限制为 –69.18 至 60.45,组内相关性为 74% (95%CI 66–80%,P < 0.001)。e-GFR 低估了 m-GFR 19.8% (95% CI 7.9–31.7%)。e-GFR 值在 m-GFR 的 10%、20% 和 30% 范围内的准确度分别为 68.3%、72.6% 和 78.8%。根据 e-GFR,24 小时内 AKI 的发生率为 60.1%,根据 m-GFR 为 54.3%(kappa 0.569,P < 0.001;敏感性为 85.8%,95%CI(78-91.7%)。
结论
修改后的 Schwartz 公式与99m Tc 标记的 DTPA 双血浆样本清除方法在计算 1 个月至 12 岁危重病儿童的 GFR 中表现出良好的一致性。在 PICU 床边应用公式时,应牢记低估 GFR。
试用注册
可在印度临床试验注册中心 (CTRI) www.ctri.nic.in访问协议。(前瞻性注册试验和注册号 CTRI/2017/10/010014)([注册日期:06/10/2017] 前瞻性注册试验。)(标题“使用二乙烯三胺五乙酸 (DTPA) 肾脏扫描测量的肾小球滤过率与估计的肾小球使用改良 Schwartz 公式对危重儿童的过滤率:一项前瞻性观察性分析研究。”)。










































 京公网安备 11010802027423号
京公网安备 11010802027423号