Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2021-09-20 , DOI: 10.1016/j.jacc.2021.07.046 James L Januzzi 1 , Faiez Zannad 2 , Stefan D Anker 3 , Javed Butler 4 , Gerasimos Filippatos 5 , Stuart J Pocock 6 , João Pedro Ferreira 7 , Naveed Sattar 8 , Subodh Verma 9 , Ola Vedin 10 , Janet Schnee 11 , Tomoko Iwata 12 , Dan Cotton 11 , Milton Packer 13 ,
|
Background
The relationship between the benefits of empagliflozin in heart failure with reduced ejection fraction (HFrEF) and N-terminal pro–B-type natriuretic peptide (NT-proBNP) has not been reported.
Objectives
The authors sought to evaluate the relationship between NT-proBNP and empagliflozin effects in EMPEROR-Reduced (Empagliflozin Outcome Trial in Patients With Chronic Heart Failure With Reduced Ejection Fraction).
Methods
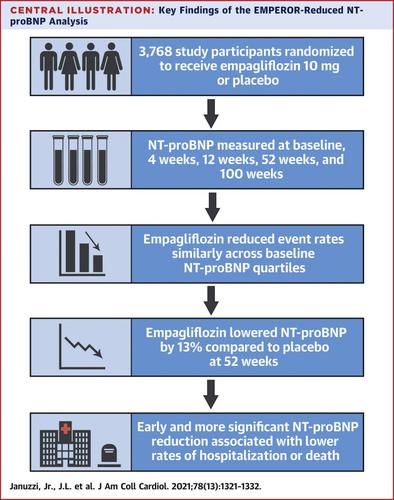
Patients with HFrEF were randomly assigned to placebo or empagliflozin 10 mg daily. NT-proBNP was measured at baseline, 4 weeks, 12 weeks, 52 weeks, and 100 weeks. Patients were divided into quartiles of baseline NT-proBNP.
Results
Incidence rates for each study outcome were 4- to 6-fold higher among those in the highest versus lowest NT-proBNP quartiles (≥3,480 vs <1,115 pg/mL). Study participants with higher NT-proBNP had 2- to 3-fold total hospitalizations higher than the lowest NT-proBNP quartile. Empagliflozin reduced risk for major cardiorenal events without heterogeneity across NT-proBNP quartiles (primary endpoint Pinteraction = 0.94; renal composite endpoint Pinteraction = 0.71). Empagliflozin treatment significantly reduced NT-proBNP at all timepoints examined; by 52 weeks, the adjusted mean difference from placebo was 13% (P < 0.001). An NT-proBNP in the lowest quartile (<1,115 pg/mL) 12 weeks after randomization was associated with lower risk for subsequent cardiovascular death or heart failure hospitalization regardless of baseline concentration. Treatment with empagliflozin resulted in 27% higher adjusted odds of an NT-proBNP concentration of <1,115 pg/mL by 12 weeks compared with placebo (P = 0.01).
Conclusions
In EMPEROR-Reduced, higher baseline NT-proBNP concentrations were associated with greater risk for adverse heart failure or renal outcomes, but empagliflozin reduced risk regardless of baseline NT-proBNP concentration. The NT-proBNP concentration after treatment with empagliflozin better informs subsequent prognosis than pretreatment concentrations. (Empagliflozin Outcome Trial in Patients With Chronic Heart Failure With Reduced Ejection Fraction [EMPEROR-Reduced]; NCT03057977)
中文翻译:
NT-proBNP 的预后重要性和 Empagliflozin 在 EMPEROR-Reduced 试验中的作用
背景
恩格列净治疗射血分数降低的心力衰竭 (HFrEF) 与 N 端 B 型利钠肽原 (NT-proBNP) 之间的关系尚未见报道。
目标
作者试图在 EMPEROR-Reduced(射血分数降低的慢性心力衰竭患者的恩格列净结局试验)中评估 NT-proBNP 与恩格列净作用之间的关系。
方法
HFrEF 患者被随机分配到安慰剂组或恩格列净组,每天 10 毫克。NT-proBNP 在基线、4 周、12 周、52 周和 100 周时测量。患者被分为基线 NT-proBNP 的四分位数。
结果
每个研究结果的发生率在最高与最低 NT-proBNP 四分位数(≥3,480 vs <1,115 pg/mL)中的发生率高 4 至 6 倍。NT-proBNP 较高的研究参与者的总住院率是 NT-proBNP 最低四分位数的 2 至 3 倍。Empagliflozin 降低了主要心肾事件的风险,且 NT-proBNP 四分位数无异质性(主要终点P相互作用 = 0.94;肾脏复合终点P相互作用 = 0.71)。在检查的所有时间点,恩格列净治疗显着降低了 NT-proBNP;到 52 周时,与安慰剂的调整后平均差异为 13% ( P < 0.001)。无论基线浓度如何,随机化后 12 周最低四分位数 (<1,115 pg/mL) 的 NT-proBNP 与随后发生心血管死亡或心力衰竭住院的风险较低相关。与安慰剂相比,恩格列净治疗导致 12 周时 NT-proBNP 浓度 <1,115 pg/mL 的调整几率高 27%(P = 0.01)。
结论
在 EMPEROR-Reduced 中,较高的基线 NT-proBNP 浓度与更大的不良心力衰竭或肾脏结局风险相关,但无论基线 NT-proBNP 浓度如何,恩格列净都能降低风险。恩格列净治疗后的 NT-proBNP 浓度比治疗前的浓度更好地为后续预后提供信息。(恩格列净对射血分数降低的慢性心力衰竭患者的结果试验 [EMPEROR-Reduced];NCT03057977)










































 京公网安备 11010802027423号
京公网安备 11010802027423号