Diabetologia ( IF 8.2 ) Pub Date : 2021-08-26 , DOI: 10.1007/s00125-021-05524-1 Tamara K Young 1 , Jing-Wei Li 1 , Amy Kang 1 , Hiddo J L Heerspink 1 , Carinna Hockham 2 , Clare Arnott 1, 3 , Brendon L Neuen 1 , Sophia Zoungas 1, 4 , Kenneth W Mahaffey 5 , Vlado Perkovic 1 , Dick de Zeeuw 6 , Greg Fulcher 3 , Bruce Neal 1 , Meg Jardine 1, 3
|
Aims/hypothesis
Type 2 diabetes mellitus can manifest over a broad clinical range, although there is no clear consensus on the categorisation of disease complexity. We assessed the effects of canagliflozin, compared with placebo, on cardiovascular and kidney outcomes in the CANagliflozin cardioVascular Assessment Study (CANVAS) Program over a range of type 2 diabetes mellitus complexity, defined separately by baseline intensity of treatment, duration of diabetes and glycaemic control.
Methods
We performed a post hoc analysis of the effects of canagliflozin on major adverse cardiovascular events (MACE) according to baseline glucose-lowering treatments (0 or 1, 2 or 3+ non-insulin glucose-lowering treatments, or insulin-based treatment), duration of diabetes (<10, 10 to 16, >16 years) and HbA1c (≤53.0 mmol/mol [<7.0%], >53.0 to 58.5 mmol/mol [>7.0% to 7.5%], >58.5 to 63.9 mmol/mol [>7.5 to 8.0%], >63.9 to 69.4 mmol/mol [8.0% to 8.5%], >69.4 to 74.9 mmol/mol [>8.5 to 9.0%] or >74.9 mmol/mol [>9.0%]). We analysed additional secondary endpoints for cardiovascular and kidney outcomes, including a combined kidney outcome of sustained 40% decline in eGFR, end-stage kidney disease or death due to kidney disease. We used Cox regression analyses and compared the constancy of HRs across subgroups by fitting an interaction term (p value for significance <0.05).
Results
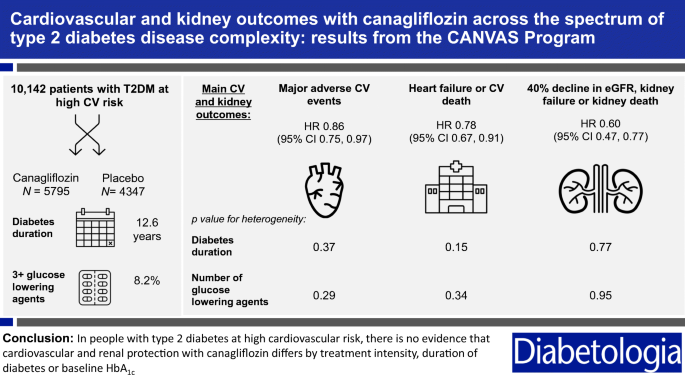
At study initiation, 5095 (50%) CANVAS Program participants were treated with insulin, 2100 (21%) had an HbA1c > 74.9 mmol/mol (9.0%) and the median duration of diabetes was 12.6 years (interquartile interval 8.0–18 years). Canagliflozin reduced MACE (HR 0.86 [95% CI 0.75, 0.97]) with no evidence that the benefit differed between subgroups defined by the number of glucose-lowering treatments, the duration of diabetes or baseline HbA1c (all p-heterogeneity >0.17). Canagliflozin reduced MACE in participants receiving insulin with no evidence that the benefit differed from other participants in the trial (HR 0.85 [95% CI 0.72, 1.00]). Similar results were observed for other cardiovascular outcomes and for the combined kidney outcome (HR for combined kidney outcome 0.60 [95% CI 0.47, 0.77]), with all p-heterogeneity >0.37.
Conclusions/interpretation
In people with type 2 diabetes mellitus at high cardiovascular risk, there was no evidence that cardiovascular and renal protection with canagliflozin differed across subgroups defined by baseline treatment intensity, duration of diabetes or HbA1c.
Graphical abstract
中文翻译:
在 HbA1c 基线水平、疾病持续时间和治疗强度不同的患者组中,卡格列净与安慰剂相比对主要不良心血管和肾脏事件的影响:来自 CANVAS 计划的结果
目标/假设
2 型糖尿病的临床表现范围很广,尽管对疾病复杂性的分类没有明确的共识。我们在 CANagliflozin 心血管评估研究 (CANVAS) 计划中评估了卡格列净与安慰剂相比对心血管和肾脏结局的影响,涵盖了一系列 2 型糖尿病复杂性,分别由基线治疗强度、糖尿病持续时间和血糖控制定义.
方法
我们根据基线降糖治疗(0 或 1、2 或 3+ 非胰岛素降糖治疗或基于胰岛素的治疗)对卡格列净对主要不良心血管事件 (MACE) 的影响进行了事后分析,糖尿病病程(<10、10 至 16、>16 年)和 HbA 1c(≤53.0 mmol/mol [<7.0%], >53.0 至 58.5 mmol/mol [>7.0% 至 7.5%], >58.5 至 63.9 mmol/mol [>7.5 至 8.0%], >63.9 至 69.4 mmol/mol [8.0% 至 8.5%]、>69.4 至 74.9 mmol/mol [>8.5 至 9.0%] 或 >74.9 mmol/mol [>9.0%])。我们分析了心血管和肾脏结果的其他次要终点,包括 eGFR 持续下降 40%、终末期肾脏疾病或肾脏疾病导致的死亡的综合肾脏结果。我们使用 Cox 回归分析并通过拟合交互项(显着性p值 <0.05)来比较亚组间 HR 的恒定性。
结果
在研究开始时,5095 名 (50%) CANVAS 计划参与者接受了胰岛素治疗,2100 名 (21%) 的 HbA 1c > 74.9 mmol/mol (9.0%),糖尿病的中位病程为 12.6 年(四分位间距 8.0-18年)。卡格列净可降低 MACE(HR 0.86 [95% CI 0.75, 0.97]),但没有证据表明由降糖治疗次数、糖尿病持续时间或基线 HbA 1c定义的亚组之间的益处存在差异(所有p-异质性> 0.17)。Canagliflozin 降低了接受胰岛素的参与者的 MACE,但没有证据表明该益处与试验中的其他参与者不同(HR 0.85 [95% CI 0.72, 1.00])。其他心血管结局和合并肾脏结局也观察到类似结果(合并肾脏结局的 HR 为 0.60 [95% CI 0.47, 0.77]),所有 p 异质性均 > 0.37。
结论/解释
在心血管风险高的 2 型糖尿病患者中,没有证据表明卡格列净对心血管和肾脏的保护作用在由基线治疗强度、糖尿病持续时间或 HbA 1c定义的亚组之间存在差异。


























 京公网安备 11010802027423号
京公网安备 11010802027423号