Atherosclerosis ( IF 4.9 ) Pub Date : 2021-08-27 , DOI: 10.1016/j.atherosclerosis.2021.08.036 Hyoungnae Kim 1 , Jung Tak Park 2 , Joongyub Lee 3 , Ji Yong Jung 4 , Kyu-Beck Lee 5 , Yeong-Hoon Kim 6 , Tae-Hyun Yoo 2 , Shin-Wook Kang 2 , Kyu Hun Choi 2 , Kook-Hwan Oh 7 , Curie Ahn 7 , Seung Hyeok Han 2 ,
|
Background and aims
Decreased kidney function is an important risk factor for cardiovascular disease (CVD). However, assessing risk of CVD may be difficult when there is a gap between creatinine- and cystatin C-based estimated glomerular filtration rate (eGFR). We studied the association of the difference in eGFRs with major adverse cardiovascular events (MACE) in patients with chronic kidney disease (CKD).
Methods
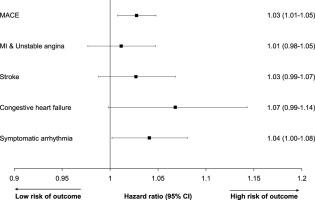
This prospective cohort study was conducted in 2076 patients with CKD stages based on the KDIGO guideline (eGFR categories of G1: ≥90; G 2: 60–89; G3: 30–59; G4: 15–29; G5: <15 mL/min/1.73 m2 without kidney replacement therapy). The difference in eGFR (eGFRdiff) was calculated by subtracting the cystatin C-based eGFR (eGFRcys) from the creatinine-based eGFR (eGFRcreat). The primary outcome was MACE, defined as non-fatal acute myocardial infarction and unstable angina, stroke, congestive heart failure, symptomatic arrhythmia, and cardiac death.
Results
During a median follow-up of 4.1 years, MACE occurred in 147 patients (incidence rate, 15.0 per 1000 patient-years). When patients were categorized into baseline eGFRdiff tertiles, the highest tertile was associated with a significantly higher risk of MACE (hazard ratio, 2.12; 95% confidence interval [CI], 1.28–3.51) than the lowest tertile when adjusted for eGFRcreat, eGFRcys, or eGFR based on both creatinine and cystatin C. Patients in the highest tertile had more baseline coronary artery calcification (CAC) than those in the lowest tertile (odds ratio [OR], 1.38; 95% CI, 1.03–1.86). In addition, 978 patients had data for both baseline and follow-up CAC at year 4. In this subgroup, baseline eGFRdiff was significantly associated with accelerated CAC progression (≥50/year) (OR, 1.03; 95% CI, 1.01–1.05).
Conclusions
A large positive difference between eGFRcreat and eGFRcys was associated with a higher risk of MACE and faster CAC progression in patients with CKD. Therefore, careful monitoring of CVD is needed for patients with a higher eGFRdiff.
中文翻译:
基于胱抑素 C 和肌酐的 eGFR 之间的差异与慢性肾病患者的不良心血管结局相关
背景和目标
肾功能下降是心血管疾病(CVD)的重要危险因素。然而,当基于肌酐和胱抑素 C 的估计肾小球滤过率 (eGFR) 之间存在差距时,评估 CVD 风险可能很困难。我们研究了慢性肾脏病 (CKD) 患者中 eGFR 差异与主要不良心血管事件 (MACE) 的关系。
方法
这项前瞻性队列研究根据 KDIGO 指南在 2076 名 CKD 分期患者中进行(eGFR 类别 G1:≥90;G 2:60-89;G3:30-59;G4:15-29;G5:<15 mL /min/1.73 m 2无肾脏替代治疗)。通过从基于肌酐的 eGFR (eGFR creat )中减去基于胱抑素 C 的 eGFR (eGFR cys ) 计算eGFR (eGFR diff ) 的差异。主要结局是 MACE,定义为非致命性急性心肌梗死和不稳定型心绞痛、中风、充血性心力衰竭、症状性心律失常和心源性死亡。
结果
在 4.1 年的中位随访期间,147 名患者发生了 MACE(发病率为 15.0/1000 患者年)。当患者被分为基线 eGFR差异三分位数时,最高三分位数的 MACE 风险显着更高(风险比,2.12;95% 置信区间 [CI],1.28-3.51)比调整 eGFR creat的最低三分位数显着更高, eGFR cys或基于肌酐和胱抑素 C 的 eGFR。最高三分位数的患者比最低三分位数的患者有更多的基线冠状动脉钙化 (CAC)(优势比 [OR],1.38;95% CI,1.03-1.86) . 此外,978 名患者在第 4 年有基线和随访 CAC 的数据。在这个亚组中,基线 eGFR差异与加速 CAC 进展(≥50/年)显着相关(OR,1.03;95% CI,1.01-1.05)。
结论
eGFR creat和 eGFR cys之间的显着正差异与 CKD 患者的 MACE 风险较高和 CAC 进展较快有关。因此,对于 eGFR差异较高的患者,需要仔细监测 CVD 。










































 京公网安备 11010802027423号
京公网安备 11010802027423号