The Journal of Thoracic and Cardiovascular Surgery ( IF 4.9 ) Pub Date : 2021-08-20 , DOI: 10.1016/j.jtcvs.2021.08.039 Jens Johansson Ramgren 1 , Igor Zindovic 2 , Shahab Nozohoor 2 , Ronny Gustafsson 2 , Nina Hakacova 3 , Johan Sjögren 2
|
Objective
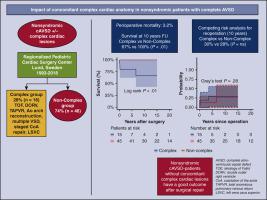
We studied a cohort of patients with nonsyndromic complete atrioventricular septal defect with and without concomitant complex cardiac anatomy and compared the outcomes after surgical repair.
Methods
Between 1993 and 2018, 62 nonsyndromic patients underwent complete atrioventricular septal defect repair. Sixteen patients (26%) had complex complete atrioventricular septal defect with variables representing concomitant cardiac anatomic complexity: tetralogy of Fallot, double outlet right ventricle, total anomalous pulmonary venous return, concomitant aortic arch reconstruction, multiple ventricular septal defects, staged repair of coarctation of the aorta, and a persisting left superior vena cava. The mean follow-up was 12.7 ± 7.9 years. Baseline variables were retrospectively evaluated and analyzed using univariable logistic regression. Survival was studied using Kaplan–Meier estimates, and group comparisons were performed using the log-rank test. A competing-risk analysis estimated the risk of reoperation with death as the competing event. A Gray's test was used to test equality of the cumulative incidence curves between groups.
Results
The perioperative mortality was 3.2% (2/62). Actuarial survival was 100% versus 66.7% ± 14.9% at 10 years in the noncomplex and complex groups, respectively (P < .01). There was no significant difference in the overall reoperation rate between the noncomplex group (7/46; 15%) and the complex group (4/16; 25%) (odds ratio, 1.86; 95% confidence interval, 0.46-7.45; P = .30). The competing-risk analysis demonstrated no significant difference in reoperation between the groups (P = .28).
Conclusions
Our data show that nonsyndromic patients without complex cardiac anatomy have a good long-term survival and an acceptable risk of reoperation similar to contemporary outcomes for patients with complete atrioventricular septal defect with trisomy 21. However, the corresponding group of nonsyndromic patients with concomitant complex cardiac lesions are still a high-risk population, especially regarding mortality.
中文翻译:
伴随复杂心脏解剖对非综合征完全性房室间隔缺损患者的影响
客观的
我们研究了一组伴有和不伴有复杂心脏解剖的非综合征性完全性房室间隔缺损患者,并比较了手术修复后的结果。
方法
1993 年至 2018 年间,62 名非综合征患者接受了完全的房室间隔缺损修复。16 名患者 (26%) 患有复杂的完全性房室间隔缺损,变量代表伴随的心脏解剖复杂性:法洛四联症、右心室双出口、完全异常肺静脉回流、伴随的主动脉弓重建、多发性室间隔缺损、分期修复主动脉和持续存在的左上腔静脉。平均随访时间为 12.7 ± 7.9 年。使用单变量逻辑回归对基线变量进行回顾性评估和分析。使用 Kaplan-Meier 估计研究生存,并使用对数秩检验进行组比较。竞争风险分析估计了以死亡为竞争事件的再手术风险。
结果
围手术期死亡率为3.2%(2/62)。非复杂组和复杂组的 10 年精算生存率分别为 100% 和 66.7% ± 14.9% ( P < . 01)。非复杂组(7/46;15%)和复杂组(4/16;25%)的总体再手术率无显着差异(优势比,1.86;95%置信区间,0.46-7.45;P = . 30)。竞争风险分析表明,各组之间的再手术无显着差异(P = .28)。
结论
我们的数据表明,没有复杂心脏解剖的非综合征患者具有良好的长期生存率和可接受的再次手术风险,与当代患有 21 三体的完全性房室间隔缺损患者的结局相似。然而,相应组的非综合征患者伴有复杂心脏病变仍然是高危人群,尤其是在死亡率方面。










































 京公网安备 11010802027423号
京公网安备 11010802027423号