Journal of the American College of Cardiology ( IF 24.0 ) Pub Date : 2021-08-16 , DOI: 10.1016/j.jacc.2021.06.028 Javier A Valle 1 , Zhuokai Li 2 , Andrzej S Kosinski 2 , Adam J Nelson 2 , Sreekanth Vemulapalli 3 , Joseph Cleveland 4 , David Fullerton 4 , John C Messenger 4 , Jessica Y Rove 4 , Rory S Bricker 4 , Steven M Bradley 5 , Frederick A Masoudi 4 , Robert W Yeh 6 , Ehrin J Armstrong 7 , Stephen W Waldo 7 , John D Carroll 4
|
Background
Societal guidelines and payor coverage decisions for transcatheter aortic valve replacement (TAVR) attempt to strike a balance between providing access and maintaining quality. The extent to which dissemination of TAVR has achieved these ideals remains unknown.
Objectives
This study sought to define patterns of TAVR dissemination in the United States and their influence on outcomes.
Methods
Using data from the TVT (Transcatheter Valvular Therapy) registry, this study identified TAVR sites from 2011 to 2018 and calculated drive-times from existing to new sites. In a contemporary cohort, this study compared site and patient characteristics by annual case volume and density of sites per million Medicare beneficiaries. Using hierarchical regression and Cox methods, this study determined the association between case volumes, site density, and changes in volume and density with patient risk profiles and outcomes.
Results
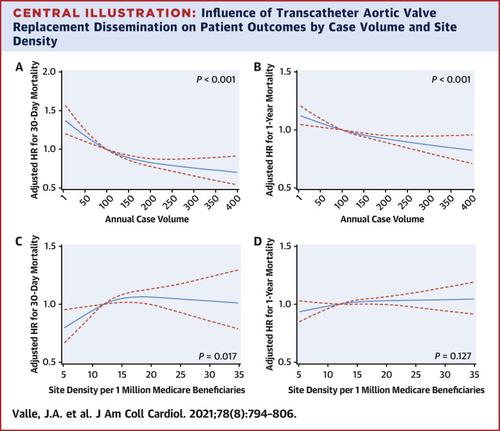
TAVR sites participating in the TVT registry increased from 198 to 556 from 2011 to 2018. Median drive-time from existing to new sites decreased from 403 minutes (interquartile range: 211-587 minutes) to 26 minutes (interquartile range: 17-48 minutes). In a contemporary cohort, higher site density was associated with lower procedural risk as well as with an increased hazard of 30-day risk-adjusted mortality (P = 0.017). Similarly, longitudinal increases in site density over time were associated with a higher hazard of 30-day (P = 0.011) and 1-year (P = 0.013) mortality.
Conclusions
TAVR has expanded significantly over time, but with regional clustering of sites. Although procedural risk is lower at higher density sites, these sites demonstrate an increased hazard of mortality. These findings suggest that the expansion of TAVR services in the United States may have had unintended consequences on procedural quality.
中文翻译:
经导管主动脉瓣置换术在美国的传播
背景
经导管主动脉瓣置换术 (TAVR) 的社会指南和付款人承保范围决定试图在提供通路和保持质量之间取得平衡。TAVR 的传播在多大程度上实现了这些理想仍然未知。
目标
本研究旨在确定美国 TAVR 传播的模式及其对结果的影响。
方法
本研究使用来自 TVT(经导管瓣膜治疗)登记的数据,确定了 2011 年至 2018 年的 TAVR 站点,并计算了从现有站点到新站点的行驶时间。在一个当代队列中,这项研究通过每年的病例数量和每百万医疗保险受益人的地点密度来比较地点和患者的特征。使用分层回归和 Cox 方法,本研究确定了病例数量、地点密度以及体积和密度变化与患者风险概况和结果之间的关联。
结果
从 2011 年到 2018 年,参与 TVT 注册的 TAVR 站点从 198 个增加到 556 个。从现有站点到新站点的中位行驶时间从 403 分钟(四分位距:211-587 分钟)减少到 26 分钟(四分位距:17-48 分钟) )。在当代队列中,较高的站点密度与较低的程序风险以及增加的 30 天风险调整死亡率风险相关(P = 0.017)。同样,随着时间的推移,场地密度的纵向增加与更高的 30 天(P = 0.011)和 1 年(P = 0.013)死亡率风险相关。
结论
随着时间的推移,TAVR 已显着扩展,但具有区域性的站点集群。尽管高密度场所的程序风险较低,但这些场所的死亡风险增加。这些发现表明,美国 TAVR 服务的扩展可能对程序质量产生了意想不到的后果。


























 京公网安备 11010802027423号
京公网安备 11010802027423号