Hepatology International ( IF 5.9 ) Pub Date : 2021-08-02 , DOI: 10.1007/s12072-021-10236-0 Chih-Horng Wu , Po-Chin Liang , Tung-Hung Su , Ming-Chi Lin , Yu-Hsuan Chang , Tiffany Ting-Fang Shih , Jia-Horng Kao
|
Background and purpose
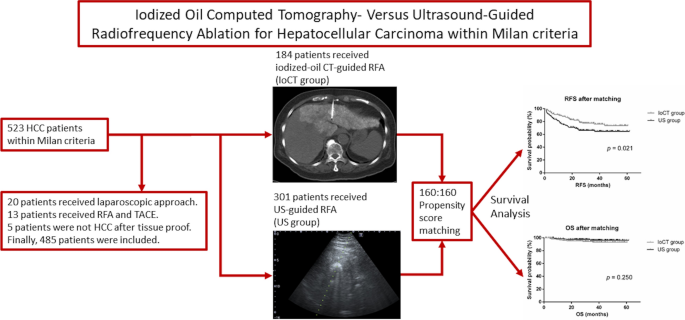
Radiofrequency ablation (RFA) is the standard of care for early stage hepatocellular carcinoma (HCC). However, the clinical outcomes of iodized oil computed tomography (IoCT) versus ultrasound (US)-guided RFA for HCC remain unclear.
Methods
We retrospectively analyzed consecutive treatment-naïve patients who received curative RFA for HCC within Milan criteria from January 2016 to December 2018. Patients who underwent either IoCT-guided RFA (IoCT group) or US-guided RFA (US group) were included. Various clinical factors, including tumor location, were adjusted with a 1:1 propensity score matching. Subsequently, the cumulative incidence rates for recurrence and hazard ratios for survival were calculated.
Results
We included 184 (37.9%) and 301 (62.1%) patients who received IoCT- and US-guided RFA, respectively. Before propensity score matching, IoCT guidance was significantly associated with multiple tumors, higher body mass index, lower albumin level, and tumors located at S8. After matching, the 1-, 2-, and 3-year local tumor progression rates of the IoCT group were significantly lower than those of the US group (4.4%, 6.9%, and 7.5% vs. 14.4%, 16.3%, and 16.3%, respectively, at p = 0.002, 0.009, and 0.016, respectively). In univariate analyses and multivariate analyses that adjusted for clinical and tumor location-related parameters, the IoCT group had better recurrence-free survival (hazard ratio = 0.581, 95% confidence interval 0.375–0.899) than those with US guidance but not overall survival.
Conclusion
IoCT-guided RFA had a lower local tumor progression rate and better recurrence-free survival than did US-guided RFA for HCC within the Milan criteria.
Graphic abstract
-
CT-guide RFA is a safe and effective alternative to US-guided with similar overall survival.
-
IoCT-guided RFA might have a better local tumor control than US-guided.
-
IoCT-guided RFA may be more suitable for male patients, aged < 70 years, a single tumor measuring 2–5 cm, and a tumor located at the subdiaphragmatic/subcardiac region.
中文翻译:
碘油计算机断层扫描对比超声引导射频消融治疗早期肝细胞癌
背景和目的
射频消融 (RFA) 是早期肝细胞癌 (HCC) 的护理标准。然而,碘油计算机断层扫描 (IoCT) 与超声 (US) 引导的 RFA 治疗 HCC 的临床结果仍不清楚。
方法
我们回顾性分析了 2016 年 1 月至 2018 年 12 月在米兰标准内接受根治性 RFA 治疗 HCC 的连续初治患者。包括接受 IoCT 引导的 RFA(IoCT 组)或美国引导的 RFA(美国组)的患者。包括肿瘤位置在内的各种临床因素通过 1:1 的倾向评分匹配进行调整。随后,计算了复发的累积发生率和生存的风险比。
结果
我们分别纳入了 184 (37.9%) 和 301 (62.1%) 名接受 IoCT 和 US 引导的 RFA 的患者。在倾向评分匹配之前,IoCT 指导与多个肿瘤、较高的体重指数、较低的白蛋白水平和位于 S8 的肿瘤显着相关。匹配后,IoCT 组的 1、2 和 3 年局部肿瘤进展率显着低于 US 组(4.4%、6.9% 和 7.5% vs. 14.4%、16.3% 和16.3%,分别为p = 0.002、0.009 和 0.016)。在针对临床和肿瘤位置相关参数进行调整的单变量分析和多变量分析中,IoCT 组的无复发生存率(风险比 = 0.581,95% 置信区间 0.375–0.899)优于美国指导组,但总体生存率不高。
结论
在米兰标准内,IoCT 引导的 RFA 比 US 引导的 RFA 治疗 HCC 具有更低的局部肿瘤进展率和更好的无复发生存率。
图形摘要
-
CT 引导 RFA 是一种安全有效的替代 US 引导,具有相似的总生存率。
-
IoCT 引导的 RFA 可能比 US 引导具有更好的局部肿瘤控制。
-
IoCT 引导的 RFA 可能更适合男性患者,年龄 < 70 岁,单个肿瘤 2-5 cm,肿瘤位于膈下/心脏下区域。










































 京公网安备 11010802027423号
京公网安备 11010802027423号