Heart Rhythm ( IF 5.6 ) Pub Date : 2021-07-30 , DOI: 10.1016/j.hrthm.2021.07.057 Marek Jastrzębski 1 , Paweł Moskal 1 , Wim Huybrechts 2 , Karol Curila 3 , Praveen Sreekumar 4 , Leonard M Rademakers 5 , Shunmuga Sundaram Ponnusamy 6 , Bengt Herweg 7 , Parikshit S Sharma 8 , Agnieszka Bednarek 1 , Marek Rajzer 1 , Pugazhendhi Vijayaraman 9
|
Background
Cardiac resynchronization therapy (CRT) based on the conventional biventricular pacing (BiV-CRT) technique sometimes results in broad QRS complex and suboptimal response.
Objective
We aimed to assess the feasibility and outcomes of CRT based on left bundle branch area pacing (LBBAP, in lieu of the right ventricular lead) combined with coronary venous left ventricular pacing in an international multicenter study.
Methods
LBBAP-optimized CRT (LOT-CRT) was attempted in nonconsecutive patients with CRT indications. Addition of the LBBA (or coronary venous) lead was at the discretion of the implanting physician, who was guided by suboptimal paced QRS complex, and/or on clinical grounds.
Results
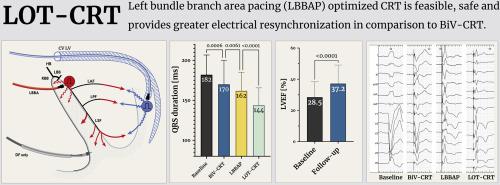
LOT-CRT was successful in 91 of 112 patients (81%). The baseline characteristics were as follows: mean age 70 ± 11 years, female 22 (20%), left ventricular ejection fraction 28.7% ± 9.8%, left ventricular end-diastolic diameter 62 ± 9 mm, N-terminal pro–B-type natriuretic peptide level 5821 ± 8193 pg/mL, left bundle branch block 47 (42%), nonspecific intraventricular conduction delay 25 (22%), right ventricular pacing 26 (23%), and right bundle branch block 14 (12%). The procedure characteristics were as follows: mean fluoroscopy time 27.3 ± 22 minutes, LBBAP capture threshold 0.8 ± 0.5 V @ 0.5 ms, and R-wave amplitude 10 mV. LOT-CRT resulted in significantly greater narrowing of QRS complex from 182 ± 25 ms at baseline to 144 ± 22 ms (P < .0001) than did BiV-CRT (170 ± 30 ms; P < .0001) and LBBAP (162 ± 23 ms; P < .0001). At follow-up of ≥3 months, the ejection fraction improved to 37% ± 12%, left ventricular end-diastolic diameter decreased to 59 ± 9 mm, N-terminal pro–B-type natriuretic peptide level decreased to 2514 ± 3537 pg/mL, pacing parameters were stable, and clinical improvement was noted in 76% of patients (New York Heart Association class 2.9 vs 1.9).
Conclusion
LOT-CRT is feasible and safe and provides greater electrical resynchronization as compared with BiV-CRT and could be an alternative, especially when only suboptimal electrical resynchronization is obtained with BiV-CRT. Randomized controlled trials comparing LOT-CRT and BiV-CRT are needed.
中文翻译:
左束支优化心脏再同步化治疗 (LOT-CRT):来自国际 LBBAP 合作研究组的结果
背景
基于传统双心室起搏 (BiV-CRT) 技术的心脏再同步化治疗 (CRT) 有时会导致宽 QRS 波群和次优反应。
客观的
我们旨在在一项国际多中心研究中评估基于左束支区域起搏(LBBAP,代替右心室导联)联合冠状静脉左心室起搏的 CRT 的可行性和结果。
方法
在有 CRT 适应症的非连续患者中尝试了 LBBAP 优化 CRT (LOT-CRT)。添加 LBBA(或冠状静脉)导联由植入医师自行决定,植入医师以次优起搏 QRS 复合波和/或临床情况为指导。
结果
LOT-CRT 在 112 名患者中的 91 名 (81%) 中成功。基线特征如下:平均年龄 70 ± 11 岁,女性 22 (20%),左心室射血分数 28.7% ± 9.8%,左心室舒张末期直径 62 ± 9 mm,N 端 pro-B 型利钠肽水平 5821 ± 8193 pg/mL,左束支传导阻滞 47 (42%),非特异性心室内传导延迟 25 (22%),右心室起搏 26 (23%),右束支传导阻滞 14 (12%)。程序特征如下:平均透视时间 27.3 ± 22 分钟,LBBAP 捕获阈值 0.8 ± 0.5 V @ 0.5 ms,R 波幅度 10 mV。与BiV-CRT (170 ± 30 ms ; P< .0001) 和 LBBAP (162 ± 23 ms; P < .0001)。随访≥3个月,射血分数提高至37%±12%,左心室舒张末期直径下降至59±9 mm,N端前B型利钠肽水平下降至2514±3537 pg /mL,起搏参数稳定,76% 的患者出现临床改善(纽约心脏协会 2.9 级 vs 1.9 级)。
结论
与 BiV-CRT 相比,LOT-CRT 是可行且安全的,并提供更大的电再同步,并且可以作为替代方案,尤其是当 BiV-CRT 仅获得次优的电再同步时。需要比较 LOT-CRT 和 BiV-CRT 的随机对照试验。










































 京公网安备 11010802027423号
京公网安备 11010802027423号