Journal of Hepatology ( IF 26.8 ) Pub Date : 2021-07-30 , DOI: 10.1016/j.jhep.2021.07.018 Gennaro D'Amico 1 , Luigi Maruzzelli 2 , Aldo Airoldi 3 , Ioannis Petridis 4 , Giulia Tosetti 5 , Antonio Rampoldi 6 , Mario D'Amico 7 , Roberto Miraglia 2 , Stella De Nicola 3 , Vincenzo La Mura 8 , Marco Solcia 6 , Riccardo Volpes 4 , Giovanni Perricone 3 , Cristiano Sgrazzutti 9 , Angelo Vanzulli 9 , Massimo Primignani 5 , Angelo Luca 2 , Giuseppe Malizia 10 , Alessandro Federico 11 , Marcello Dallio 11 , Angelo Andriulli 12 , Angelo Iacobellis 12 , Luigi Addario 13 , Matteo Garcovich 14 , Antonio Gasbarrini 14 , Luchino Chessa 15 , Francesco Salerno 16 , Giulia Gobbo 16 , Manuela Merli 17 , Lorenzo Ridola 18 , Gianluca Svegliati Baroni 19 , Giuseppe Tarantino 19 , Nicola Caporaso 20 , Filomena Morisco 20 , Pietro Pozzoni 21 , Agostino Colli 21 , Luca Saverio Belli 3
|
Background & Aims
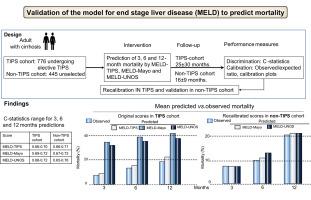
Although the discriminative ability of the model for end-stage liver disease (MELD) score is generally considered acceptable, its calibration is still unclear. In a validation study, we assessed the discriminative performance and calibration of 3 versions of the model: original MELD-TIPS, used to predict survival after transjugular intrahepatic portosystemic shunt (TIPS); classic MELD-Mayo; and MELD-UNOS, used by the United Network for Organ Sharing (UNOS). We also explored recalibrating and updating the model.
Methods
In total, 776 patients who underwent elective TIPS (TIPS cohort) and 445 unselected patients (non-TIPS cohort) were included. Three, 6 and 12-month mortality predictions were calculated by the 3 MELD versions: discrimination was assessed by c-statistics and calibration by comparing deciles of predicted and observed risks. Cox and Fine and Grey models were used for recalibration and prognostic analyses.
Results
In the TIPS/non-TIPS cohorts, the etiology of liver disease was viral in 402/188, alcoholic in 185/130, and non-alcoholic steatohepatitis in 65/33; mean follow-up±SD was 25±9/19±21 months; and the number of deaths at 3-6-12 months was 57-102-142/31-47-99, respectively. C-statistics ranged from 0.66 to 0.72 in TIPS and 0.66 to 0.76 in non-TIPS cohorts across prediction times and scores. A post hoc analysis revealed worse c-statistics in non-viral cirrhosis with more pronounced and significant worsening in the non-TIPS cohort. Calibration was acceptable with MELD-TIPS but largely unsatisfactory with MELD-Mayo and -UNOS whose performance improved much after recalibration. A prognostic analysis showed that age, albumin, and TIPS indication might be used to update the MELD.
Conclusions
In this validation study, the performance of the MELD score was largely unsatisfactory, particularly in non-viral cirrhosis. MELD recalibration and candidate variables for an update to the MELD score are proposed.
Lay summary
While the discriminative performance of the model for end-stage liver disease (MELD) score is credited to be fair to good, its calibration, the correspondence of observed to predicted mortality, is still unsettled. We found that application of 3 different versions of the MELD in 2 independent cirrhosis cohorts yielded largely imprecise mortality predictions particularly in non-viral cirrhosis. Thus, we propose a recalibration and suggest candidate variables for an update to the model.
中文翻译:
终末期肝病评分模型在死亡率预测中的表现和病因学的潜在作用
背景与目标
虽然模型对终末期肝病(MELD)评分的判别能力普遍被认为是可以接受的,但其校准仍不清楚。在一项验证研究中,我们评估了 3 个版本的模型的判别性能和校准:原始 MELD-TIPS,用于预测经颈静脉肝内门体分流术 (TIPS) 后的存活率;经典的 MELD-Mayo;器官共享联合网络 (UNOS) 使用的 MELD-UNOS。我们还探索了重新校准和更新模型。
方法
总共包括 776 名接受选择性 TIPS 的患者(TIPS 队列)和 445 名未选择的患者(非 TIPS 队列)。三个、6 个月和 12 个月的死亡率预测由 3 个 MELD 版本计算:通过 c 统计评估歧视,通过比较预测风险和观察风险的十分位数进行校准。Cox 和 Fine 和 Gray 模型用于重新校准和预后分析。
结果
在 TIPS/非 TIPS 队列中,肝病的病因是病毒性 402/188,酒精性 185/130,非酒精性脂肪性肝炎 65/33;平均随访时间±标准差为 25±9/19±21 个月;3-6-12个月的死亡人数分别为57-102-142/31-47-99。跨预测时间和分数的 C 统计量在 TIPS 中为 0.66 至 0.72,在非 TIPS 队列中为 0.66 至 0.76。事后分析显示,非病毒性肝硬化的c 统计数据更差,非 TIPS 队列的恶化更为明显和显着。MELD-TIPS 的校准是可以接受的,但 MELD-Mayo 和 -UNOS 的校准在很大程度上不能令人满意,它们的性能在重新校准后得到了很大改善。预后分析表明,年龄、白蛋白和 TIPS 指示可用于更新 MELD。
结论
在这项验证研究中,MELD 评分的表现在很大程度上不能令人满意,特别是在非病毒性肝硬化中。提出了用于更新 MELD 分数的 MELD 重新校准和候选变量。
总结
虽然终末期肝病 (MELD) 评分模型的判别性能被认为是公平到好的,但它的校准,即观察到的死亡率与预测死亡率的对应关系,仍未解决。我们发现,在 2 个独立的肝硬化队列中应用 3 种不同版本的 MELD,得出的死亡率预测在很大程度上不准确,特别是在非病毒性肝硬化中。因此,我们建议重新校准并建议更新模型的候选变量。










































 京公网安备 11010802027423号
京公网安备 11010802027423号