JACC: Heart Failure ( IF 10.3 ) Pub Date : 2021-07-07 , DOI: 10.1016/j.jchf.2021.05.007 Robert J Mentz 1 , David J Whellan 2 , Gordon R Reeves 3 , Amy M Pastva 4 , Pamela Duncan 5 , Bharathi Upadhya 6 , M Benjamin Nelson 6 , Haiying Chen 7 , Shelby D Reed 8 , Paul B Rosenberg 1 , Alain G Bertoni 9 , Christopher M O'Connor 10 , Dalane W Kitzman 11
|
Objectives
This study assessed for treatment interactions by ejection fraction (EF) subgroup (≥45% [heart failure with preserved ejection fraction (HFpEF); vs <45% [heart failure with reduced ejection fraction (HFrEF)]).
Background
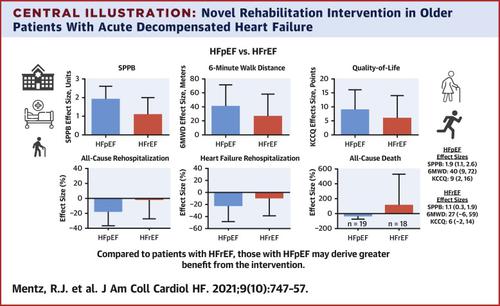
The REHAB-HF trial showed that an early multidomain rehabilitation intervention improved physical function, frailty, quality-of-life, and depression in older patients hospitalized with acute decompensated heart failure (ADHF).
Methods
Three-month outcomes were: Short Physical Performance Battery (SPPB), 6-min walk distance (6MWD), and Kansas City Cardiomyopathy Questionnaire (KCCQ). Six-month end points included all-cause rehospitalization and death and a global rank of death, all-cause rehospitalization, and SPPB. Prespecified significance level for interaction was P ≤ 0.1.
Results
Among 349 total participants, 185 (53%) had HFpEF and 164 (47%) had HFrEF. Compared with HFrEF, HFpEF participants were more often women (61% vs 43%) and had significantly worse baseline physical function, frailty, quality of life, and depression. Although interaction P values for 3-month outcomes were not significant, effect sizes were larger for HFpEF vs HFrEF: SPPB +1.9 (95% CI: 1.1-2.6) vs +1.1 (95% CI: 0.3-1.9); 6MWD +40 meters (95% CI: 9 meters-72 meters) vs +27 (95% CI: −6 meters to 59 meters); KCCQ +9 (2-16) vs +6 (−2 to 14). All-cause rehospitalization rate was nominally lower with intervention in HFpEF but not HFrEF [effect size 0.83 (95% CI: 0.64-1.09) vs 0.99 (95% CI: 0.74-1.33); interaction P = 0.40]. There were significantly greater treatment benefits in HFpEF vs HFrEF for all-cause death [interaction P = 0.08; intervention rate ratio 0.63 (95% CI: 0.25-1.61) vs 2.21 (95% CI: 0.78-6.25)], and the global rank end point (interaction P = 0.098) with benefit seen in HFpEF [probability index 0.59 (95% CI: 0.50-0.68)] but not HFrEF.
Conclusions
Among older patients hospitalized with ADHF, compared with HFrEF those with HFpEF had significantly worse impairments at baseline and may derive greater benefit from the intervention. (A Trial of Rehabilitation Therapy in Older Acute Heart Failure Patients [REHAB-HF]; NCT02196038)
中文翻译:
保留射血分数与减少射血分数的老年急性心力衰竭患者的康复干预
目标
本研究通过射血分数 (EF) 亚组评估治疗相互作用(≥45% [射血分数保留的心力衰竭 (HFpEF);vs <45% [射血分数降低的心力衰竭 (HFrEF)])。
背景
REHAB-HF 试验表明,早期多领域康复干预可改善因急性失代偿性心力衰竭 (ADHF) 住院的老年患者的身体功能、虚弱、生活质量和抑郁。
方法
三个月的结果是:短体能电池 (SPPB)、6 分钟步行距离 (6MWD) 和堪萨斯城心肌病问卷 (KCCQ)。六个月的终点包括全因再住院和死亡以及全球死亡等级、全因再住院和 SPPB。交互作用的预设显着性水平为P ≤ 0.1。
结果
在 349 名参与者中,185 人(53%)患有 HFpEF,164 人(47%)患有 HFrEF。与 HFrEF 相比,HFpEF 参与者更多是女性(61% 对 43%),并且基线身体功能、虚弱、生活质量和抑郁症明显更差。尽管 3 个月结果的交互P值不显着,但 HFpEF 与 HFrEF 的影响大小更大:SPPB +1.9 (95% CI: 1.1-2.6) vs +1.1 (95% CI: 0.3-1.9);6MWD +40 米(95% CI:9 米至 72 米)对比 +27(95% CI:-6 米至 59 米);KCCQ +9(2-16)对 +6(-2 到 14)。干预 HFpEF 而不是 HFrEF 干预的全因再住院率名义上较低[效应大小 0.83 (95% CI: 0.64-1.09) 对比 0.99 (95% CI: 0.74-1.33);交互P =0.40]。对于全因死亡,HFpEF 与 HFrEF 相比有显着更大的治疗益处 [交互作用P = 0.08;干预率比 0.63 (95% CI: 0.25-1.61) vs 2.21 (95% CI: 0.78-6.25)],全球排名终点(交互P = 0.098)在 HFpEF [概率指数 0.59 (95% CI: 0.50-0.68)] 但不是 HFrEF。
结论
在因 ADHF 住院的老年患者中,与 HFrEF 相比,HFpEF 患者的基线损伤明显更差,并且可能从干预中获得更大的益处。(老年急性心力衰竭患者的康复治疗试验 [REHAB-HF];NCT02196038)










































 京公网安备 11010802027423号
京公网安备 11010802027423号