JACC: Heart Failure ( IF 13.0 ) Pub Date : 2021-07-07 , DOI: 10.1016/j.jchf.2021.05.008 Peter S Pang 1 , Frances M Russell 1 , Robert Ehrman 2 , Rob Ferre 1 , Luna Gargani 3 , Phillip D Levy 2 , Vicki Noble 4 , Kathleen A Lane 5 , Xiaochun Li 5 , Sean P Collins 6
|
Objectives
The goal of this study was to determine whether a 6-hour lung ultrasound (LUS)-guided strategy-of-care improves pulmonary congestion over usual management in the emergency department (ED) setting. A secondary goal was to explore whether early targeted intervention leads to improved outcomes.
Background
Targeting pulmonary congestion in acute heart failure remains a key goal of care. LUS B-lines are a semi-quantitative assessment of pulmonary congestion. Whether B-lines decrease in patients with acute heart failure by targeting therapy is not well known.
Methods
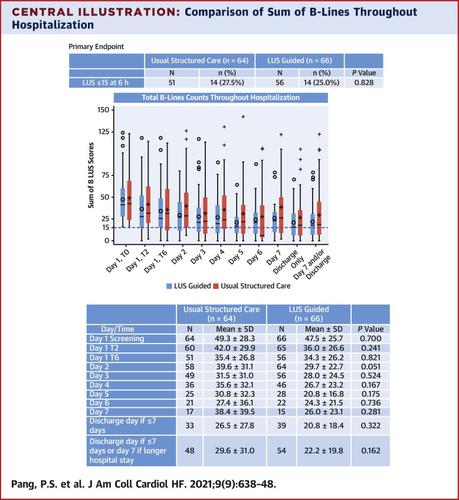
A multicenter, single-blind, ED-based, pilot trial randomized 130 patients to receive a 6-hour LUS-guided treatment strategy versus structured usual care. Patients were followed up throughout hospitalization and 90 days’ postdischarge. B-lines ≤15 at 6 h was the primary outcome, and days alive and out of hospital (DAOOH) at 30 days was the main exploratory outcome.
Results
No significant difference in the proportion of patients with B-lines ≤15 at 6 hours (25.0% LUS vs 27.5% usual care; P = 0.83) or the number of B-lines at 6 hours (35.4 ± 26.8 LUS vs 34.3 ± 26.2 usual care; P = 0.82) was observed between groups. There were also no differences in DAOOH (21.3 ± 6.6 LUS vs 21.3 ± 7.1 usual care; P = 0.99). However, a significantly greater reduction in the number of B-lines was observed in LUS-guided patients compared with those receiving usual structured care during the first 48 hours (P = 0.04).
Conclusions
In this pilot trial, ED use of LUS to target pulmonary congestion conferred no benefit compared with usual care in reducing the number of B-lines at 6 hours or in 30 days DAOOH. However, LUS-guided patients had faster resolution of congestion during the initial 48 hours. (B-lines Lung Ultrasound–Guided ED Management of Acute Heart Failure Pilot Trial; NCT03136198)
中文翻译:
肺超声指导的急性心力衰竭急诊科管理 (BLUSHED-AHF)
目标
本研究的目的是确定 6 小时肺部超声 (LUS) 指导的护理策略是否比急诊科 (ED) 环境中的常规管理改善肺充血。次要目标是探索早期有针对性的干预是否能改善结果。
背景
针对急性心力衰竭的肺充血仍然是护理的一个关键目标。LUS B 线是肺充血的半定量评估。靶向治疗是否会降低急性心力衰竭患者的 B 线尚不清楚。
方法
一项多中心、单盲、基于 ED 的试点试验随机分配 130 名患者接受 6 小时 LUS 指导的治疗策略与结构化常规护理。在整个住院期间和出院后 90 天对患者进行随访。6 小时时 B 线≤15 是主要结果,30 天时的存活天数和出院天数 (DAOOH) 是主要探索性结果。
结果
6 小时时 B 线≤15 的患者比例(25.0% LUS 对 27.5% 常规治疗;P = 0.83)或 6 小时 B 线数量(35.4 ± 26.8 LUS 对 34.3 ± 26.2)没有显着差异常规护理;P = 0.82)在组间观察到。DAOOH 也没有差异(21.3 ± 6.6 LUS 对比 21.3 ± 7.1 常规护理;P = 0.99)。然而,与在最初 48 小时内接受常规结构化护理的患者相比,在 LUS 指导下的患者中观察到 B 线数量显着减少(P = 0.04)。
结论
在这项试点试验中,与常规护理相比,ED 使用 LUS 治疗肺充血在减少 6 小时或 30 天 DAOOH 的 B 线数量方面没有任何益处。然而,LUS 引导的患者在最初的 48 小时内可以更快地缓解充血。(B 线肺超声引导 ED 管理急性心力衰竭试点试验;NCT03136198)


























 京公网安备 11010802027423号
京公网安备 11010802027423号