Archives of Cardiovascular Diseases ( IF 2.3 ) Pub Date : 2021-04-29 , DOI: 10.1016/j.acvd.2021.01.004 Florent Arregle 1 , Helene Martel 1 , Mary Philip 1 , Frederique Gouriet 2 , Jean Paul Casalta 2 , Alberto Riberi 3 , Olivier Torras 1 , Anne-Claire Casalta 1 , Laurence Camoin-Jau 4 , Flora Lavagna 1 , Sebastien Renard 1 , Pierre Ambrosi 1 , Hubert Lepidi 2 , Frederic Collart 3 , Sandrine Hubert 1 , Michel Drancourt 2 , Didier Raoult 2 , Gilbert Habib 5
|
Background
Infective endocarditis (IE) is associated with a high mortality rate, related in part to neurological complications. Studies suggest that valvular surgery should be performed early when indicated, but is often delayed by the presence of neurological complications.
Aim
To assess the effect of delaying surgery in patients with IE and neurological complications and to identify factors predictive of death.
Methods
In a prospective, single-centre study in a referral centre for IE, all patients with IE underwent systematic screening for neurological complications. The primary outcome was 6-month death. In patients presenting with neurological complications, the prognosis according to surgical status was analysed and a Cox regression model used to identify variables predictive of death.
Results
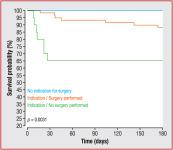
Between April 2014 and January 2018, 351 patients with a definite diagnosis of left-sided IE were included. Ninety-four patients (26.8%) presented with at least one neurological complication. Fifty-nine patients (17.7%) died during 6-month follow-up. Six-month mortality rates did not differ significantly between patients with and without neurological complications (P = 0.60). Forty patients had a temporary surgical contraindication because of neurological complications. During the period of surgical contraindication, seven of these patients (17.5%) died, six (15.0%) presented a new embolic event, and 12 (30.0%) presented cardiac or septic deterioration. In multivariable analysis, predictive factors of death in patients presenting with neurological complications were temporary surgical contraindication (hazard ratio 7.36, 95% confidence interval 1.61–33.67; P = 0.010) and presence of a mechanical prosthetic valve (hazard ratio 16.40, 95% confidence interval 2.22–121.17; P = 0.006).
Conclusions
Patients with a temporary surgical contraindication due to neurological complications had a higher risk of death and frequent major complications while waiting for surgery. When indicated, the decision to postpone surgery in the early phase should be weighed against the risk of infectious or cardiac deterioration.
中文翻译:
伴有神经系统并发症的感染性心内膜炎:延迟心脏手术与较差的预后相关
背景
感染性心内膜炎 (IE) 与高死亡率有关,部分与神经系统并发症有关。研究表明,瓣膜手术应在有指征时及早进行,但往往因出现神经系统并发症而延迟。
目的
评估延迟手术对 IE 和神经系统并发症患者的影响,并确定预测死亡的因素。
方法
在 IE 转诊中心的一项前瞻性、单中心研究中,所有 IE 患者都接受了神经系统并发症的系统筛查。主要结果是 6 个月的死亡。在出现神经系统并发症的患者中,根据手术状态分析预后,并使用 Cox 回归模型确定预测死亡的变量。
结果
2014 年 4 月至 2018 年 1 月期间,共纳入 351 名确诊为左侧 IE 的患者。94 名患者 (26.8%) 出现至少一种神经系统并发症。59 名患者 (17.7%) 在 6 个月的随访期间死亡。有和没有神经系统并发症的患者的 6 个月死亡率没有显着差异(P = 0.60)。由于神经系统并发症,40 名患者有暂时的手术禁忌症。在手术禁忌期间,这些患者中有 7 名 (17.5%) 死亡,6 名 (15.0%) 出现新的栓塞事件,12 名 (30.0%) 出现心脏或脓毒症恶化。在多变量分析中,出现神经系统并发症的患者死亡的预测因素是暂时的手术禁忌症(风险比 7.36,95% 置信区间 1.61–33.67;P = 0.010)和机械瓣膜的存在(风险比 16.40,95% 置信度)间隔 2.22–121.17;P = 0.006)。
结论
由于神经系统并发症而存在临时手术禁忌症的患者在等待手术期间死亡风险较高,并且经常出现严重并发症。如有需要,早期推迟手术的决定应与感染或心脏恶化的风险进行权衡。










































 京公网安备 11010802027423号
京公网安备 11010802027423号