当前位置:
X-MOL 学术
›
J. Neuroendocrinol.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Surgery of the primary tumour in 201 patients with high-grade gastroenteropancreatic neuroendocrine and mixed neuroendocrine-non-neuroendocrine neoplasms
Journal of Neuroendocrinology ( IF 3.3 ) Pub Date : 2021-03-26 , DOI: 10.1111/jne.12967 Hans-Christian Pommergaard 1, 2 , Kirstine Nielsen 1, 2, 3 , Halfdan Sorbye 4, 5 , Birgitte Federspiel 1, 6 , Elizaveta M Tabaksblat 7, 8 , Lene W Vestermark 9 , Eva T Janson 10, 11 , Carsten P Hansen 1, 2 , Morten Ladekarl 7, 8, 12 , Herish Garresori 13 , Geir O Hjortland 14, 15 , Anna Sundlöv 16 , Renate Galleberg 4 , Pauline Knigge 1, 3, 17 , Andreas Kjaer 1, 17 , Seppo W Langer 1, 18 , Ulrich Knigge 1, 2, 3
Journal of Neuroendocrinology ( IF 3.3 ) Pub Date : 2021-03-26 , DOI: 10.1111/jne.12967 Hans-Christian Pommergaard 1, 2 , Kirstine Nielsen 1, 2, 3 , Halfdan Sorbye 4, 5 , Birgitte Federspiel 1, 6 , Elizaveta M Tabaksblat 7, 8 , Lene W Vestermark 9 , Eva T Janson 10, 11 , Carsten P Hansen 1, 2 , Morten Ladekarl 7, 8, 12 , Herish Garresori 13 , Geir O Hjortland 14, 15 , Anna Sundlöv 16 , Renate Galleberg 4 , Pauline Knigge 1, 3, 17 , Andreas Kjaer 1, 17 , Seppo W Langer 1, 18 , Ulrich Knigge 1, 2, 3
Affiliation
|
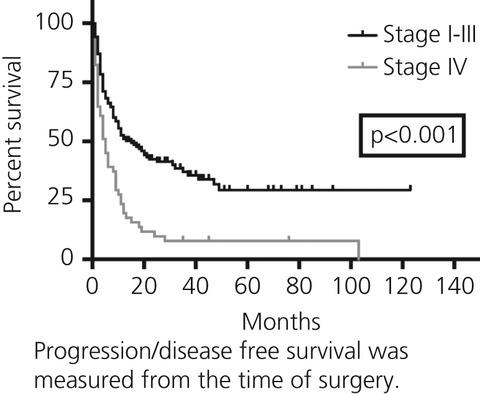
The benefit of surgery in high-grade gastroenteropancreatic neuroendocrine neoplasms (GEP NEN) and mixed neuroendocrine-non-neuroendocrine neoplasms (MiNEN) is uncertain. The present study aimed to investigate outcomes after tumour surgery in patients with high-grade (Ki-67 > 20%) GEP NEN or MiNEN stage I-III or stage IV. We analysed data from patients treated in the period 2007-2015 at eight Nordic university hospitals. Overall survival (OS) and progression-free survival (PFS)/disease-free survival (DFS) were analysed by Kaplan-Meier estimates. Prognostic factors were evaluated using Cox regression. We included 201 surgically resected patients, 143 stage I-III and 58 stage IV, with 68% having neuroendocrine carcinoma, 23% MiNEN, 5% neuroendocrine tumour G3 and 4% uncertain NEN G3. Primary tumours were located in colon/rectum (52%), oesophagus/cardia (19%), pancreas (10%), stomach (7%), jejunum/ileum (5%), duodenum (4%), gallbladder (2%) and anal canal (1%). For patients with stage I-III, median DFS was 12 months (95% confidence interval [CI] = 5.5-18.5) and median OS was 32 months (95% CI = 24.0-40.0). For patients with stage I-III and an R0 resection, median DFS was 21 months (95% CI = 4.9-37.1) and median OS was 39 months (95% CI = 25.0-53.0). For patients with stage IV, median PFS/DFS was 4 months (95% CI = 1.9-6.1) and median OS was 11 months (95% CI = 4.8-17.2). For patients with stage IV and an R0 resection, median DFS was 6 months (95% CI = 0-16.4) and median OS was 32 months (95% CI = 25.5-38.5). Performance status > 1 and colorectal primary were associated with poor prognosis. There was no difference in survival between patients with high-grade GEP NEN and MiNEN. Surgery of the primary tumour in patients with loco-regional high-grade GEP NEN or MiNEN led to good long-term results and should be considered if an R0 resection is considered achievable. Highly selected patients with stage IV disease may also benefit from surgery.
中文翻译:

201例高级别胃肠胰神经内分泌及神经内分泌-非神经内分泌混合肿瘤患者的原发肿瘤手术
高级别胃肠胰腺神经内分泌肿瘤 (GEP NEN) 和混合性神经内分泌-非神经内分泌肿瘤 (MiNEN) 的手术益处尚不确定。本研究旨在调查高级别(Ki-67 > 20%)GEP NEN 或 MiNEN I-III 期或 IV 期患者肿瘤手术后的结果。我们分析了 2007-2015 年期间在北欧八家大学医院接受治疗的患者的数据。通过 Kaplan-Meier 估计分析总生存期 (OS) 和无进展生存期 (PFS)/无病生存期 (DFS)。使用 Cox 回归评估预后因素。我们纳入了 201 名手术切除的患者,143 名 I-III 期和 58 名 IV 期患者,其中 68% 患有神经内分泌癌,23% 患有 MiNEN,5% 患有神经内分泌肿瘤 G3 和 4% 不确定 NEN G3。原发性肿瘤位于结肠/直肠(52%),食道/贲门 (19%)、胰腺 (10%)、胃 (7%)、空肠/回肠 (5%)、十二指肠 (4%)、胆囊 (2%) 和肛管 (1%)。对于 I-III 期患者,中位 DFS 为 12 个月(95% 置信区间 [CI] = 5.5-18.5),中位 OS 为 32 个月(95% CI = 24.0-40.0)。对于 I-III 期和 R0 切除的患者,中位 DFS 为 21 个月(95% CI = 4.9-37.1),中位 OS 为 39 个月(95% CI = 25.0-53.0)。对于 IV 期患者,中位 PFS/DFS 为 4 个月(95% CI = 1.9-6.1),中位 OS 为 11 个月(95% CI = 4.8-17.2)。对于 IV 期和 R0 切除的患者,中位 DFS 为 6 个月(95% CI = 0-16.4),中位 OS 为 32 个月(95% CI = 25.5-38.5)。体能状态 > 1 和结直肠原发与预后不良相关。高级别 GEP NEN 和 MiNEN 患者的生存率没有差异。对局部区域高级别 GEP NEN 或 MiNEN 患者进行原发肿瘤手术可产生良好的长期结果,如果认为可以实现 R0 切除,则应考虑手术。高度选择的 IV 期疾病患者也可能从手术中受益。
更新日期:2021-05-25
中文翻译:
201例高级别胃肠胰神经内分泌及神经内分泌-非神经内分泌混合肿瘤患者的原发肿瘤手术
高级别胃肠胰腺神经内分泌肿瘤 (GEP NEN) 和混合性神经内分泌-非神经内分泌肿瘤 (MiNEN) 的手术益处尚不确定。本研究旨在调查高级别(Ki-67 > 20%)GEP NEN 或 MiNEN I-III 期或 IV 期患者肿瘤手术后的结果。我们分析了 2007-2015 年期间在北欧八家大学医院接受治疗的患者的数据。通过 Kaplan-Meier 估计分析总生存期 (OS) 和无进展生存期 (PFS)/无病生存期 (DFS)。使用 Cox 回归评估预后因素。我们纳入了 201 名手术切除的患者,143 名 I-III 期和 58 名 IV 期患者,其中 68% 患有神经内分泌癌,23% 患有 MiNEN,5% 患有神经内分泌肿瘤 G3 和 4% 不确定 NEN G3。原发性肿瘤位于结肠/直肠(52%),食道/贲门 (19%)、胰腺 (10%)、胃 (7%)、空肠/回肠 (5%)、十二指肠 (4%)、胆囊 (2%) 和肛管 (1%)。对于 I-III 期患者,中位 DFS 为 12 个月(95% 置信区间 [CI] = 5.5-18.5),中位 OS 为 32 个月(95% CI = 24.0-40.0)。对于 I-III 期和 R0 切除的患者,中位 DFS 为 21 个月(95% CI = 4.9-37.1),中位 OS 为 39 个月(95% CI = 25.0-53.0)。对于 IV 期患者,中位 PFS/DFS 为 4 个月(95% CI = 1.9-6.1),中位 OS 为 11 个月(95% CI = 4.8-17.2)。对于 IV 期和 R0 切除的患者,中位 DFS 为 6 个月(95% CI = 0-16.4),中位 OS 为 32 个月(95% CI = 25.5-38.5)。体能状态 > 1 和结直肠原发与预后不良相关。高级别 GEP NEN 和 MiNEN 患者的生存率没有差异。对局部区域高级别 GEP NEN 或 MiNEN 患者进行原发肿瘤手术可产生良好的长期结果,如果认为可以实现 R0 切除,则应考虑手术。高度选择的 IV 期疾病患者也可能从手术中受益。









































 京公网安备 11010802027423号
京公网安备 11010802027423号