当前位置:
X-MOL 学术
›
J. Am. Coll. Cardiol.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Prevalence and Outcomes of Concomitant Aortic Stenosis and Cardiac Amyloidosis
Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2021-01-01 , DOI: 10.1016/j.jacc.2020.11.006 Christian Nitsche 1 , Paul R Scully 2 , Kush P Patel 3 , Andreas A Kammerlander 1 , Matthias Koschutnik 1 , Carolina Dona 1 , Tim Wollenweber 4 , Nida Ahmed 3 , George D Thornton 3 , Andrew D Kelion 5 , Nikant Sabharwal 5 , James D Newton 5 , Muhiddin Ozkor 6 , Simon Kennon 6 , Michael Mullen 6 , Guy Lloyd 7 , Marianna Fontana 8 , Philip N Hawkins 8 , Francesca Pugliese 9 , Leon J Menezes 10 , James C Moon 3 , Julia Mascherbauer 1 , Thomas A Treibel 3
Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2021-01-01 , DOI: 10.1016/j.jacc.2020.11.006 Christian Nitsche 1 , Paul R Scully 2 , Kush P Patel 3 , Andreas A Kammerlander 1 , Matthias Koschutnik 1 , Carolina Dona 1 , Tim Wollenweber 4 , Nida Ahmed 3 , George D Thornton 3 , Andrew D Kelion 5 , Nikant Sabharwal 5 , James D Newton 5 , Muhiddin Ozkor 6 , Simon Kennon 6 , Michael Mullen 6 , Guy Lloyd 7 , Marianna Fontana 8 , Philip N Hawkins 8 , Francesca Pugliese 9 , Leon J Menezes 10 , James C Moon 3 , Julia Mascherbauer 1 , Thomas A Treibel 3
Affiliation
|
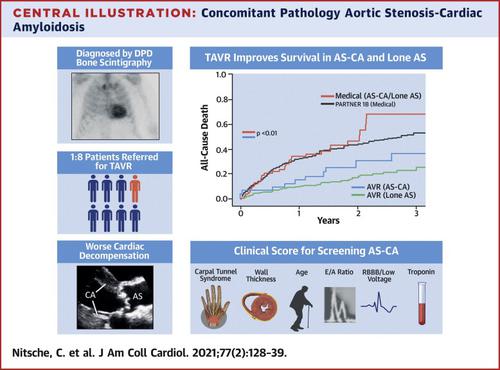
Background Older patients with severe aortic stenosis (AS) are increasingly identified as having cardiac amyloidosis (CA). It is unknown whether concomitant AS-CA has worse outcomes or results in futility of transcatheter aortic valve replacement (TAVR). Objectives This study identified clinical characteristics and outcomes of AS-CA compared with lone AS. Methods Patients who were referred for TAVR at 3 international sites underwent blinded research core laboratory 99mtechnetium-3,3-diphosphono-1,2-propanodicarboxylic acid (DPD) bone scintigraphy (Perugini grade 0: negative; grades 1 to 3: increasingly positive) before intervention. Transthyretin-CA (ATTR) was diagnosed by DPD and absence of a clonal immunoglobulin, and light-chain CA (AL) was diagnosed via tissue biopsy. National registries captured all-cause mortality. Results A total of 407 patients (age 83.4 ± 6.5 years; 49.8% men) were recruited. DPD was positive in 48 patients (11.8%; grade 1: 3.9% [n = 16]; grade 2/3: 7.9% [n = 32]). AL was diagnosed in 1 patient with grade 1. Patients with grade 2/3 had worse functional capacity, biomarkers (N-terminal pro-brain natriuretic peptide and/or high-sensitivity troponin T), and biventricular remodeling. A clinical score (RAISE) that used left ventricular remodeling (hypertrophy/diastolic dysfunction), age, injury (high-sensitivity troponin T), systemic involvement, and electrical abnormalities (right bundle branch block/low voltages) was developed to predict the presence of AS-CA (area under the curve: 0.86; 95% confidence interval: 0.78 to 0.94; p < 0.001). Decisions by the heart team (DPD-blinded) resulted in TAVR (333 [81.6%]), surgical AVR (10 [2.5%]), or medical management (65 [15.9%]). After a median of 1.7 years, 23% of patients died. One-year mortality was worse in all patients with AS-CA (grade: 1 to 3) than those with lone AS (24.5% vs. 13.9%; p = 0.05). TAVR improved survival versus medical management; AS-CA survival post-TAVR did not differ from lone AS (p = 0.36). Conclusions Concomitant pathology of AS-CA is common in older patients with AS and can be predicted clinically. AS-CA has worse clinical presentation and a trend toward worse prognosis, unless treated. Therefore, TAVR should not be withheld in AS-CA.
中文翻译:

并发主动脉瓣狭窄和心脏淀粉样变性的患病率和结果
背景 患有严重主动脉瓣狭窄(AS)的老年患者越来越多地被认为患有心脏淀粉样变性(CA)。目前尚不清楚伴随的 AS-CA 是否会产生更差的结果或导致经导管主动脉瓣置换术 (TAVR) 无效。目的 本研究确定了 AS-CA 与单纯 AS 相比的临床特征和结果。方法 对在 3 个国际地点转诊进行 TAVR 的患者进行盲法研究核心实验室 99m锝-3,3-二膦酰基-1,2-丙二甲酸 (DPD) 骨闪烁扫描(Perugini 0 级:阴性;1 至 3 级:阳性增加)干预前。运甲状腺素蛋白-CA (ATTR) 通过 DPD 和克隆免疫球蛋白缺失进行诊断,轻链 CA (AL) 通过组织活检进行诊断。国家登记处记录了全因死亡率。结果 总共招募了 407 名患者(年龄 83.4 ± 6.5 岁;49.8% 为男性)。48 名患者 DPD 呈阳性(11.8%;1 级:3.9% [n = 16];2/3 级:7.9% [n = 32])。1 例 1 级患者被诊断为 AL。2/3 级患者的功能能力、生物标志物(N 端脑钠肽前体和/或高敏肌钙蛋白 T)和双心室重塑较差。临床评分 (RAISE) 使用左心室重构(肥厚/舒张功能障碍)、年龄、损伤(高敏肌钙蛋白 T)、全身受累和电异常(右束支传导阻滞/低电压)来预测其存在AS-CA(曲线下面积:0.86;95% 置信区间:0.78 至 0.94;p < 0.001)。心脏团队(DPD 盲法)做出的决定包括 TAVR (333 [81.6%])、手术 AVR (10 [2.5%]) 或药物治疗 (65 [15.9%])。平均 1.7 年后,23% 的患者死亡。所有 AS-CA 患者(1 至 3 级)的一年死亡率均比单纯 AS 患者差(24.5% vs. 13.9%;p = 0.05)。与医疗管理相比,TAVR 提高了生存率;TAVR 后 AS-CA 生存率与单独 AS 没有差异 (p = 0.36)。结论 AS-CA 的伴随病理在老年 AS 患者中很常见,并且可以在临床上预测。如果不进行治疗,AS-CA 的临床表现会更差,且预后有更差的趋势。因此,AS-CA 不应保留 TAVR。
更新日期:2021-01-01
中文翻译:
并发主动脉瓣狭窄和心脏淀粉样变性的患病率和结果
背景 患有严重主动脉瓣狭窄(AS)的老年患者越来越多地被认为患有心脏淀粉样变性(CA)。目前尚不清楚伴随的 AS-CA 是否会产生更差的结果或导致经导管主动脉瓣置换术 (TAVR) 无效。目的 本研究确定了 AS-CA 与单纯 AS 相比的临床特征和结果。方法 对在 3 个国际地点转诊进行 TAVR 的患者进行盲法研究核心实验室 99m锝-3,3-二膦酰基-1,2-丙二甲酸 (DPD) 骨闪烁扫描(Perugini 0 级:阴性;1 至 3 级:阳性增加)干预前。运甲状腺素蛋白-CA (ATTR) 通过 DPD 和克隆免疫球蛋白缺失进行诊断,轻链 CA (AL) 通过组织活检进行诊断。国家登记处记录了全因死亡率。结果 总共招募了 407 名患者(年龄 83.4 ± 6.5 岁;49.8% 为男性)。48 名患者 DPD 呈阳性(11.8%;1 级:3.9% [n = 16];2/3 级:7.9% [n = 32])。1 例 1 级患者被诊断为 AL。2/3 级患者的功能能力、生物标志物(N 端脑钠肽前体和/或高敏肌钙蛋白 T)和双心室重塑较差。临床评分 (RAISE) 使用左心室重构(肥厚/舒张功能障碍)、年龄、损伤(高敏肌钙蛋白 T)、全身受累和电异常(右束支传导阻滞/低电压)来预测其存在AS-CA(曲线下面积:0.86;95% 置信区间:0.78 至 0.94;p < 0.001)。心脏团队(DPD 盲法)做出的决定包括 TAVR (333 [81.6%])、手术 AVR (10 [2.5%]) 或药物治疗 (65 [15.9%])。平均 1.7 年后,23% 的患者死亡。所有 AS-CA 患者(1 至 3 级)的一年死亡率均比单纯 AS 患者差(24.5% vs. 13.9%;p = 0.05)。与医疗管理相比,TAVR 提高了生存率;TAVR 后 AS-CA 生存率与单独 AS 没有差异 (p = 0.36)。结论 AS-CA 的伴随病理在老年 AS 患者中很常见,并且可以在临床上预测。如果不进行治疗,AS-CA 的临床表现会更差,且预后有更差的趋势。因此,AS-CA 不应保留 TAVR。










































 京公网安备 11010802027423号
京公网安备 11010802027423号