当前位置:
X-MOL 学术
›
J. Am. Coll. Cardiol.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Implications of Alternative Definitions of Peri-Procedural Myocardial Infarction After Coronary Revascularization
Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2020-10-01 , DOI: 10.1016/j.jacc.2020.08.016 John Gregson , Gregg W. Stone , Ori Ben-Yehuda , Björn Redfors , David E. Kandzari , Marie-Claude Morice , Martin B. Leon , Ioanna Kosmidou , Nicholas J. Lembo , W. Morris Brown , Dimitri Karmpaliotis , Adrian P. Banning , Jose Pomar , Manel Sabaté , Charles A. Simonton , Ovidiu Dressler , Arie Pieter Kappetein , Joseph F. Sabik , Patrick W. Serruys , Stuart J. Pocock
Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2020-10-01 , DOI: 10.1016/j.jacc.2020.08.016 John Gregson , Gregg W. Stone , Ori Ben-Yehuda , Björn Redfors , David E. Kandzari , Marie-Claude Morice , Martin B. Leon , Ioanna Kosmidou , Nicholas J. Lembo , W. Morris Brown , Dimitri Karmpaliotis , Adrian P. Banning , Jose Pomar , Manel Sabaté , Charles A. Simonton , Ovidiu Dressler , Arie Pieter Kappetein , Joseph F. Sabik , Patrick W. Serruys , Stuart J. Pocock
|
BACKGROUND
Varying definitions of procedural myocardial infarction (PMI) are in widespread use. OBJECTIVES
This study sought to determine the rates and clinical relevance of PMI using different definitions in patients with left main coronary artery disease randomized to percutaneous coronary intervention (PCI) versus coronary artery bypass grafting (CABG) surgery in the EXCEL (Evaluation of XIENCE versus Coronary Artery Bypass Surgery for Effectiveness of Left Main Revascularization) trial. METHODS
The pre-specified protocol definition of PMI (PMIProt) required a large elevation of creatine kinase-MB (CK-MB), with identical threshold for both procedures. The Third Universal Definition of MI (types 4a and 5) (PMIUD) required lesser biomarker elevations but with supporting evidence of myocardial ischemia, different after PCI and CABG. For the PMIUD, troponins were used preferentially (available in 49.5% of patients), CK-MB otherwise. The multivariable relationship between each PMI type and 5-year mortality was determined. RESULTS
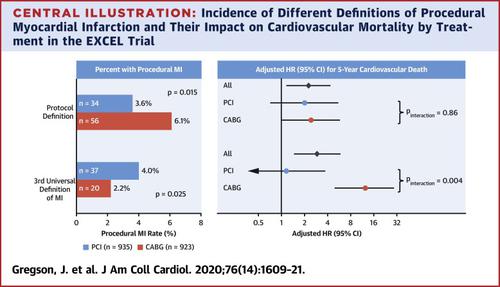
PMIProt occurred in 34 of 935 (3.6%) patients after PCI and 56 of 923 (6.1%) patients after CABG (difference -2.4%; 95% confidence interval [CI]: -4.4% to -0.5%; p = 0.015). The corresponding rates of PMIUD were 37 (4.0%) and 20 (2.2%), respectively (difference 1.8%; 95% CI: 0.2% to 3.4%; p = 0.025). Both PMIProt and PMIUD were associated with 5-year cardiovascular mortality (adjusted hazard ratio [HR]: 2.18 [95% CI: 1.13 to 4.23] and 2.87 [95% CI: 1.44 to 5.73], respectively). PMIProt was associated with a consistent hazard of cardiovascular mortality after both PCI and CABG (pinteraction = 0.86). Conversely, PMIUD was strongly associated with cardiovascular mortality after CABG (adjusted HR: 11.94; 95% CI: 4.84 to 29.47) but not after PCI (adjusted HR: 1.14; 95% CI: 0.35 to 3.67) (pinteraction = 0.004). Results were similar for all-cause mortality and with varying PMIUD biomarker definitions. Only large biomarker elevations (CK-MB ≥10× upper reference limit and troponin ≥70× upper reference limit) were associated with mortality. CONCLUSIONS
The rates of PMI after PCI and CABG vary greatly with different definitions. In the EXCEL trial, the pre-specified PMIProt was associated with similar hazard after PCI and CABG, whereas PMIUD was strongly associated with mortality after CABG but not after PCI. (EXCEL Clinical Trial [EXCEL]; NCT01205776).
中文翻译:

冠状动脉血运重建后围手术期心肌梗死的替代定义的意义
背景广泛使用对程序性心肌梗塞(PMI)的不同定义。目的 本研究试图在 EXCEL(XIENCE 与冠状动脉的评估)中随机接受经皮冠状动脉介入治疗 (PCI) 与冠状动脉旁路移植术 (CABG) 手术的左主干冠状动脉疾病患者中使用不同的定义来确定 PMI 的发生率和临床相关性。动脉搭桥手术对左主干血运重建的有效性)试验。方法 PMI (PMIProt) 的预先指定协议定义需要肌酸激酶-MB (CK-MB) 的大幅升高,两个程序的阈值相同。MI(4a 型和 5 型)(PMIUD)的第三个通用定义需要较少的生物标志物升高,但有心肌缺血的支持证据,在 PCI 和 CABG 后有所不同。对于 PMIUD,优先使用肌钙蛋白(49.5% 的患者可用),否则使用 CK-MB。确定了每种 PMI 类型与 5 年死亡率之间的多变量关系。结果 PCI 后 935 名患者中有 34 名 (3.6%) 出现 PMIProt,CABG 后 923 名患者中有 56 名 (6.1%) 出现 PMIProt(差异 -2.4%;95% 置信区间 [CI]:-4.4% 至 -0.5%;p = 0.015 )。相应的 PMIUD 率分别为 37 (4.0%) 和 20 (2.2%)(差异 1.8%;95% CI:0.2% 至 3.4%;p = 0.025)。PMIProt 和 PMIUD 均与 5 年心血管死亡率相关(调整后的风险比 [HR]:2.18 [95% CI:1.13 至 4.23] 和 2.87 [95% CI:1.44 至 5.73])。PMIProt 与 PCI 和 CABG 后一致的心血管死亡风险相关(pinteraction = 0.86)。反过来,PMIUD 与 CABG 后的心血管死亡率密切相关(调整后的 HR:11.94;95% CI:4.84 至 29.47),但与 PCI 后无关(调整后的 HR:1.14;95% CI:0.35 至 3.67)(交互作用 = 0.004)。全因死亡率和不同 PMIUD 生物标志物定义的结果相似。只有较大的生物标志物升高(CK-MB ≥ 10 × 参考上限和肌钙蛋白 ≥ 70 × 参考上限)与死亡率相关。结论 PCI和CABG术后PMI发生率因定义不同而差异很大。在 EXCEL 试验中,预先指定的 PMIProt 与 PCI 和 CABG 后相似的风险相关,而 PMIUD 与 CABG 后死亡率密切相关,但与 PCI 后死亡率无关。(EXCEL 临床试验 [EXCEL];NCT01205776)。35 到 3.67)(pinteraction = 0.004)。全因死亡率和不同 PMIUD 生物标志物定义的结果相似。只有较大的生物标志物升高(CK-MB ≥ 10 × 参考上限和肌钙蛋白 ≥ 70 × 参考上限)与死亡率相关。结论 PCI和CABG术后PMI发生率因定义不同而差异较大。在 EXCEL 试验中,预先指定的 PMIProt 与 PCI 和 CABG 后相似的风险相关,而 PMIUD 与 CABG 后死亡率密切相关,但与 PCI 后死亡率无关。(EXCEL 临床试验 [EXCEL];NCT01205776)。35 到 3.67)(pinteraction = 0.004)。全因死亡率和不同 PMIUD 生物标志物定义的结果相似。只有较大的生物标志物升高(CK-MB ≥ 10 × 参考上限和肌钙蛋白 ≥ 70 × 参考上限)与死亡率相关。结论 PCI和CABG术后PMI发生率因定义不同而差异很大。在 EXCEL 试验中,预先指定的 PMIProt 与 PCI 和 CABG 后相似的风险相关,而 PMIUD 与 CABG 后死亡率密切相关,但与 PCI 后死亡率无关。(EXCEL 临床试验 [EXCEL];NCT01205776)。结论 PCI和CABG术后PMI发生率因定义不同而差异较大。在 EXCEL 试验中,预先指定的 PMIProt 与 PCI 和 CABG 后相似的风险相关,而 PMIUD 与 CABG 后死亡率密切相关,但与 PCI 后死亡率无关。(EXCEL 临床试验 [EXCEL];NCT01205776)。结论 PCI和CABG术后PMI发生率因定义不同而差异较大。在 EXCEL 试验中,预先指定的 PMIProt 与 PCI 和 CABG 后相似的风险相关,而 PMIUD 与 CABG 后死亡率密切相关,但与 PCI 后死亡率无关。(EXCEL 临床试验 [EXCEL];NCT01205776)。
更新日期:2020-10-01
中文翻译:
冠状动脉血运重建后围手术期心肌梗死的替代定义的意义
背景广泛使用对程序性心肌梗塞(PMI)的不同定义。目的 本研究试图在 EXCEL(XIENCE 与冠状动脉的评估)中随机接受经皮冠状动脉介入治疗 (PCI) 与冠状动脉旁路移植术 (CABG) 手术的左主干冠状动脉疾病患者中使用不同的定义来确定 PMI 的发生率和临床相关性。动脉搭桥手术对左主干血运重建的有效性)试验。方法 PMI (PMIProt) 的预先指定协议定义需要肌酸激酶-MB (CK-MB) 的大幅升高,两个程序的阈值相同。MI(4a 型和 5 型)(PMIUD)的第三个通用定义需要较少的生物标志物升高,但有心肌缺血的支持证据,在 PCI 和 CABG 后有所不同。对于 PMIUD,优先使用肌钙蛋白(49.5% 的患者可用),否则使用 CK-MB。确定了每种 PMI 类型与 5 年死亡率之间的多变量关系。结果 PCI 后 935 名患者中有 34 名 (3.6%) 出现 PMIProt,CABG 后 923 名患者中有 56 名 (6.1%) 出现 PMIProt(差异 -2.4%;95% 置信区间 [CI]:-4.4% 至 -0.5%;p = 0.015 )。相应的 PMIUD 率分别为 37 (4.0%) 和 20 (2.2%)(差异 1.8%;95% CI:0.2% 至 3.4%;p = 0.025)。PMIProt 和 PMIUD 均与 5 年心血管死亡率相关(调整后的风险比 [HR]:2.18 [95% CI:1.13 至 4.23] 和 2.87 [95% CI:1.44 至 5.73])。PMIProt 与 PCI 和 CABG 后一致的心血管死亡风险相关(pinteraction = 0.86)。反过来,PMIUD 与 CABG 后的心血管死亡率密切相关(调整后的 HR:11.94;95% CI:4.84 至 29.47),但与 PCI 后无关(调整后的 HR:1.14;95% CI:0.35 至 3.67)(交互作用 = 0.004)。全因死亡率和不同 PMIUD 生物标志物定义的结果相似。只有较大的生物标志物升高(CK-MB ≥ 10 × 参考上限和肌钙蛋白 ≥ 70 × 参考上限)与死亡率相关。结论 PCI和CABG术后PMI发生率因定义不同而差异很大。在 EXCEL 试验中,预先指定的 PMIProt 与 PCI 和 CABG 后相似的风险相关,而 PMIUD 与 CABG 后死亡率密切相关,但与 PCI 后死亡率无关。(EXCEL 临床试验 [EXCEL];NCT01205776)。35 到 3.67)(pinteraction = 0.004)。全因死亡率和不同 PMIUD 生物标志物定义的结果相似。只有较大的生物标志物升高(CK-MB ≥ 10 × 参考上限和肌钙蛋白 ≥ 70 × 参考上限)与死亡率相关。结论 PCI和CABG术后PMI发生率因定义不同而差异较大。在 EXCEL 试验中,预先指定的 PMIProt 与 PCI 和 CABG 后相似的风险相关,而 PMIUD 与 CABG 后死亡率密切相关,但与 PCI 后死亡率无关。(EXCEL 临床试验 [EXCEL];NCT01205776)。35 到 3.67)(pinteraction = 0.004)。全因死亡率和不同 PMIUD 生物标志物定义的结果相似。只有较大的生物标志物升高(CK-MB ≥ 10 × 参考上限和肌钙蛋白 ≥ 70 × 参考上限)与死亡率相关。结论 PCI和CABG术后PMI发生率因定义不同而差异很大。在 EXCEL 试验中,预先指定的 PMIProt 与 PCI 和 CABG 后相似的风险相关,而 PMIUD 与 CABG 后死亡率密切相关,但与 PCI 后死亡率无关。(EXCEL 临床试验 [EXCEL];NCT01205776)。结论 PCI和CABG术后PMI发生率因定义不同而差异较大。在 EXCEL 试验中,预先指定的 PMIProt 与 PCI 和 CABG 后相似的风险相关,而 PMIUD 与 CABG 后死亡率密切相关,但与 PCI 后死亡率无关。(EXCEL 临床试验 [EXCEL];NCT01205776)。结论 PCI和CABG术后PMI发生率因定义不同而差异较大。在 EXCEL 试验中,预先指定的 PMIProt 与 PCI 和 CABG 后相似的风险相关,而 PMIUD 与 CABG 后死亡率密切相关,但与 PCI 后死亡率无关。(EXCEL 临床试验 [EXCEL];NCT01205776)。










































 京公网安备 11010802027423号
京公网安备 11010802027423号