当前位置:
X-MOL 学术
›
J. Am. Coll. Cardiol.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Nonculprit Lesion Severity and Outcome of Revascularization in Patients With STEMI and Multivessel Coronary Disease
Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2020-09-01 , DOI: 10.1016/j.jacc.2020.07.034 Tej Sheth 1 , Natalia Pinilla-Echeverri 1 , Raul Moreno 2 , Jia Wang 1 , David A Wood 3 , Robert F Storey 4 , Roxana Mehran 5 , Kevin R Bainey 6 , Matthias Bossard 7 , Sripal Bangalore 8 , Jon-David Schwalm 1 , James L Velianou 9 , Nicholas Valettas 9 , Matthew Sibbald 9 , Josep Rodés-Cabau 10 , John Ducas 11 , Eric A Cohen 12 , Akshay Bagai 13 , Stephane Rinfret 14 , David E Newby 15 , Laurent Feldman 16 , Steven B Laster 17 , Irene M Lang 18 , Joseph D Mills 19 , John A Cairns 3 , Shamir R Mehta 1
Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2020-09-01 , DOI: 10.1016/j.jacc.2020.07.034 Tej Sheth 1 , Natalia Pinilla-Echeverri 1 , Raul Moreno 2 , Jia Wang 1 , David A Wood 3 , Robert F Storey 4 , Roxana Mehran 5 , Kevin R Bainey 6 , Matthias Bossard 7 , Sripal Bangalore 8 , Jon-David Schwalm 1 , James L Velianou 9 , Nicholas Valettas 9 , Matthew Sibbald 9 , Josep Rodés-Cabau 10 , John Ducas 11 , Eric A Cohen 12 , Akshay Bagai 13 , Stephane Rinfret 14 , David E Newby 15 , Laurent Feldman 16 , Steven B Laster 17 , Irene M Lang 18 , Joseph D Mills 19 , John A Cairns 3 , Shamir R Mehta 1
Affiliation
|
BACKGROUND
In the COMPLETE (Complete vs Culprit-only Revascularization to Treat Multi-vessel Disease After Early PCI for STEMI) trial, angiography-guided percutaneous coronary intervention (PCI) of nonculprit lesions with the aim of complete revascularization reduced major cardiovascular (CV) events in patients with ST-segment elevation myocardial infarction (MI) and multivessel coronary artery disease. OBJECTIVES
The purpose of this study was to determine the effect of nonculprit-lesion stenosis severity measured by quantitative coronary angiography (QCA) on the benefit of complete revascularization. METHODS
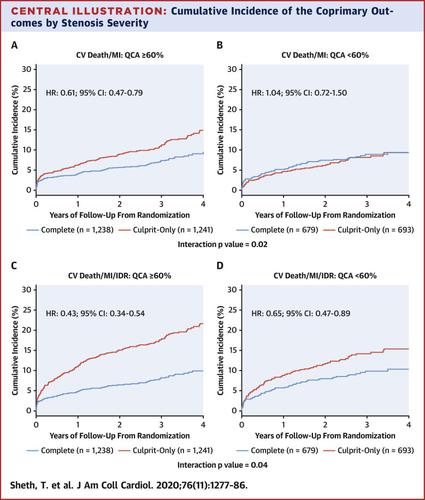
Among 4,041 patients randomized in the COMPLETE trial, nonculprit lesion stenosis severity was measured using QCA in the angiographic core laboratory in 3,851 patients with 5,355 nonculprit lesions. In pre-specified analyses, the treatment effect in patients with QCA stenosis ≥60% versus <60% on the first coprimary outcome of CV death or new MI and the second co-primary outcome of CV death, new MI, or ischemia-driven revascularization was determined. RESULTS
The first coprimary outcome was reduced with complete revascularization in the 2,479 patients with QCA stenosis ≥60% (2.5%/year vs. 4.2%/year; hazard ratio [HR]: 0.61; 95% confidence interval [CI]: 0.47 to 0.79), but not in the 1,372 patients with QCA stenosis <60% (3.0%/year vs. 2.9%/year; HR: 1.04; 95% CI: 0.72 to 1.50; interaction p = 0.02). The second coprimary outcome was reduced in patients with QCA stenosis ≥60% (2.9%/year vs. 6.9%/year; HR: 0.43; 95% CI: 0.34 to 0.54) to a greater extent than patients with QCA stenosis <60% (3.3%/year vs. 5.2%/year; HR: 0.65; 95% CI: 0.47 to 0.89; interaction p = 0.04). CONCLUSIONS
Among patients with ST-segment elevation MI and multivessel coronary artery disease, complete revascularization reduced major CV outcomes to a greater extent in patients with stenosis severity of ≥60% compared with <60%, as determined by quantitative coronary angiography.
中文翻译:

STEMI 和多支冠状动脉疾病患者的非肇事病变严重程度和血运重建结果
背景 在 COMPLET(针对 STEMI 早期 PCI 后进行完全血运重建与仅罪犯血运重建治疗多支血管疾病)试验中,血管造影引导下的非罪犯病变经皮冠状动脉介入治疗 (PCI) 旨在完全血运重建,减少主要心血管 (CV) 事件ST 段抬高型心肌梗塞 (MI) 和多支冠状动脉疾病患者。目的 本研究的目的是确定通过定量冠状动脉造影 (QCA) 测量的非罪犯病变狭窄严重程度对完全血运重建获益的影响。方法 在 COMPLETE 试验中随机分配的 4,041 名患者中,在血管造影核心实验室使用 QCA 测量了 3,851 名患者的非罪犯病变狭窄严重程度,其中 5,355 个非罪犯病变。在预先指定的分析中,QCA 狭窄 ≥60% 与 <60% 的患者对 CV 死亡或新发 MI 的第一个共同主要结局以及 CV 死亡、新发 MI 或缺血驱动的第二个共同主要结局的治疗效果确定了血运重建。结果 2,479 名 QCA 狭窄≥60% 的患者中,随着完全血运重建,第一个主要结果降低(2.5%/年 vs. 4.2%/年;风险比 [HR]:0.61;95% 置信区间 [CI]:0.47 至0.79),但在 1,372 名 QCA 狭窄 <60% 的患者中则不然(3.0%/年 vs. 2.9%/年;HR:1.04;95% CI:0.72 至 1.50;交互作用 p = 0.02)。QCA 狭窄≥60% 的患者的第二个共同主要结局比 QCA 狭窄 <60% 的患者降低程度更大(2.9%/年 vs. 6.9%/年;HR:0.43;95% CI:0.34 至 0.54) (3.3%/年 vs. 5.2%/年;HR:0.65;95% CI:0.47 至 0.89;交互作用 p = 0.04)。结论 在 ST 段抬高型心肌梗死和多支冠状动脉疾病的患者中,根据定量冠状动脉造影确定,与狭窄严重程度≥60% 的患者相比,完全血运重建可更大程度地降低主要心血管结局。
更新日期:2020-09-01
中文翻译:
STEMI 和多支冠状动脉疾病患者的非肇事病变严重程度和血运重建结果
背景 在 COMPLET(针对 STEMI 早期 PCI 后进行完全血运重建与仅罪犯血运重建治疗多支血管疾病)试验中,血管造影引导下的非罪犯病变经皮冠状动脉介入治疗 (PCI) 旨在完全血运重建,减少主要心血管 (CV) 事件ST 段抬高型心肌梗塞 (MI) 和多支冠状动脉疾病患者。目的 本研究的目的是确定通过定量冠状动脉造影 (QCA) 测量的非罪犯病变狭窄严重程度对完全血运重建获益的影响。方法 在 COMPLETE 试验中随机分配的 4,041 名患者中,在血管造影核心实验室使用 QCA 测量了 3,851 名患者的非罪犯病变狭窄严重程度,其中 5,355 个非罪犯病变。在预先指定的分析中,QCA 狭窄 ≥60% 与 <60% 的患者对 CV 死亡或新发 MI 的第一个共同主要结局以及 CV 死亡、新发 MI 或缺血驱动的第二个共同主要结局的治疗效果确定了血运重建。结果 2,479 名 QCA 狭窄≥60% 的患者中,随着完全血运重建,第一个主要结果降低(2.5%/年 vs. 4.2%/年;风险比 [HR]:0.61;95% 置信区间 [CI]:0.47 至0.79),但在 1,372 名 QCA 狭窄 <60% 的患者中则不然(3.0%/年 vs. 2.9%/年;HR:1.04;95% CI:0.72 至 1.50;交互作用 p = 0.02)。QCA 狭窄≥60% 的患者的第二个共同主要结局比 QCA 狭窄 <60% 的患者降低程度更大(2.9%/年 vs. 6.9%/年;HR:0.43;95% CI:0.34 至 0.54) (3.3%/年 vs. 5.2%/年;HR:0.65;95% CI:0.47 至 0.89;交互作用 p = 0.04)。结论 在 ST 段抬高型心肌梗死和多支冠状动脉疾病的患者中,根据定量冠状动脉造影确定,与狭窄严重程度≥60% 的患者相比,完全血运重建可更大程度地降低主要心血管结局。










































 京公网安备 11010802027423号
京公网安备 11010802027423号