Clinical Gastroenterology and Hepatology ( IF 11.6 ) Pub Date : 2020-07-02 , DOI: 10.1016/j.cgh.2020.06.046 Sun Woong Kim 1 , Jun Sik Yoon 2 , Junyong Park 3 , Yong Jin Jung 4 , Jae Seung Lee 3 , Jisoo Song 4 , Han Ah Lee 5 , Yeon Seok Seo 5 , Minjong Lee 6 , Jin Myung Park 6 , Dae Hee Choi 6 , Moon Young Kim 7 , Seong Hee Kang 7 , Jin Mo Yang 8 , Do Seon Song 8 , Sung Won Chung 9 , Minseok Albert Kim 9 , Hee Joon Jang 9 , Hyunwoo Oh 9 , Cheol-Hyung Lee 9 , Yun Bin Lee 9 , Eun Ju Cho 9 , Su Jong Yu 9 , Yoon Jun Kim 9 , Jung-Hwan Yoon 9 , Jeong-Hoon Lee 9
|
Background & Aims
Third-generation cephalosporins (TGCs) are recommended as first-line antibiotics for treatment of spontaneous bacterial peritonitis (SBP). However, antibiotics against multidrug-resistant organisms (such as carbapenems) might be necessary. We aimed to evaluate whether carbapenems are superior to TGC for treatment of SBP.
Methods
We performed a retrospective study of 865 consecutive patients with a first presentation of SBP (275 culture positive; 103 with TGC-resistant bacterial infections) treated at 7 referral centers in Korea, from September 2013 through January 2018. The primary outcome was in-hospital mortality. We made all comparisons using data from patients whose baseline characteristics were balanced by inverse probability of treatment weighting.
Results
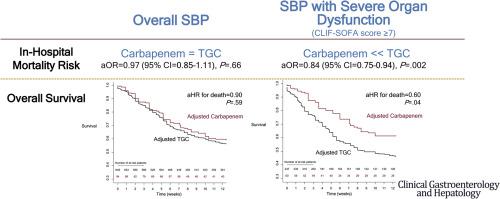
Of patients who initially received empirical treatment with antibiotics, 95 (11.0%) received carbapenems and 655 (75.7%) received TGCs. Among the entire study cohort, there was no significant difference in in-hospital mortality between the carbapenem (25.8%) and TGC (25.3%) groups (adjusted odds ratio [aOR], 0.97; 95% CI, 0.85–1.11; P = .66). In the subgroup of patients with high chronic liver failure-sequential organ failure assessment (CLIF-SOFA) scores (score of 7 or greater, n = 314), carbapenem treatment was associated with lower in-hospital mortality (23.1%) than in the TGC group (38.8%) (aOR, 0.84; 95% CI, 0.75–0.94; P=.002). In contrast, among patients with lower CLIF-SOFA scores (n = 436), in-hospital mortality did not differ significantly between the carbapenem group (24.7%) and the TGC group (16.0%) (aOR, 1.06; 95% CI, 0.85–1.32; P = .58).
Conclusions
For patients with a first presentation of SBP, empirical treatment with carbapenem does not reduce in-hospital mortality compared to treatment with TGCs. However, among critically ill patients (CLIF-SOFA scores ≥7), empirical carbapenem treatment was significantly associated with lower in-hospital mortality than TGCs.
中文翻译:
碳青霉烯与第三代头孢菌素治疗自发性细菌性腹膜炎的经验性治疗
背景与目标
第三代头孢菌素 (TGC) 被推荐作为治疗自发性细菌性腹膜炎 (SBP) 的一线抗生素。然而,针对多重耐药菌(如碳青霉烯类)的抗生素可能是必要的。我们旨在评估碳青霉烯类药物治疗 SBP 是否优于 TGC。
方法
我们对 2013 年 9 月至 2018 年 1 月在韩国 7 个转诊中心接受治疗的 865 名首次出现 SBP 的连续患者(275 名培养阳性;103 名患有 TGC 耐药细菌感染)进行了一项回顾性研究。主要结果是住院期间死亡率。我们使用来自基线特征通过治疗加权的逆概率平衡的患者的数据进行所有比较。
结果
在最初接受抗生素经验治疗的患者中,95 名 (11.0%) 接受碳青霉烯类治疗,655 名 (75.7%) 接受 TGC。在整个研究队列中,碳青霉烯 (25.8%) 和 TGC (25.3%) 组之间的院内死亡率没有显着差异(调整后的优势比 [aOR],0.97;95% CI,0.85-1.11;P = .66)。在慢性肝衰竭-序贯器官衰竭评估 (CLIF-SOFA) 评分较高(7 分或更高,n = 314)的患者亚组中,碳青霉烯类治疗与较低的院内死亡率(23.1%)相关TGC 组 (38.8%) (aOR, 0.84; 95% CI, 0.75–0.94; P=.002)。相比之下,在 CLIF-SOFA 评分较低的患者 (n = 436) 中,碳青霉烯组 (24.7%) 和 TGC 组 (16.0%) 的院内死亡率没有显着差异(aOR,1.06;95% CI, 0.85–1.32;P = .58)。
结论
对于首次出现 SBP 的患者,与 TGC 治疗相比,碳青霉烯经验性治疗不会降低院内死亡率。然而,在危重患者中(CLIF-SOFA 评分≥7),经验性碳青霉烯类治疗与较低的院内死亡率显着相关。










































 京公网安备 11010802027423号
京公网安备 11010802027423号