JAMA Neurology ( IF 20.4 ) Pub Date : 2020-06-01 , DOI: 10.1001/jamaneurol.2020.0319 Michael V Mazya 1, 2 , Annika Berglund 1, 2 , Niaz Ahmed 1, 2 , Mia von Euler 3, 4 , Staffan Holmin 2, 5 , Ann-Charlotte Laska 6 , Jan M Mathé 2, 7 , Christina Sjöstrand 1, 2 , Einar E Eriksson 1, 2
|
Importance To our knowledge, it is unknown whether a prehospital stroke triage system combining symptom severity and teleconsultation could accurately select patients for primary stroke center bypass and hasten delivery of endovascular thrombectomy (EVT) without delaying intravenous thrombolysis (IVT).
Objective To evaluate the predictive performance of the newly implemented Stockholm Stroke Triage System (SSTS) for large-artery occlusion (LAO) stroke and EVT initiation. Secondary objectives included evaluating whether the Stockholm Stroke Triage System shortened onset-to-puncture time for EVT and onset-to-needle time (ONT) for IVT.
Design, Setting, and Participants This population-based prospective cohort study conducted from October 2017 to October 2018 across the Stockholm region (Sweden) included patients transported by first-priority (“code stroke”) ambulance to the hospital for acute stroke suspected by an ambulance nurse and historical controls (October 2016-October 2017). Exclusion criteria were in-hospital stroke and helicopter or private transport. Of 2909 eligible patients, 4 (0.14%) declined participation.
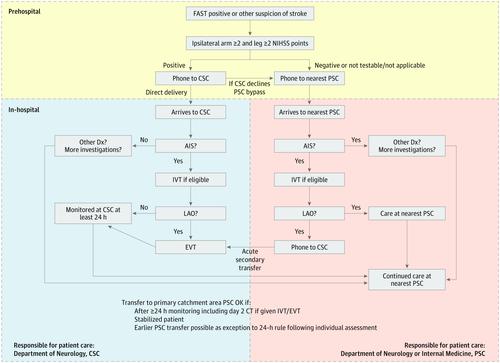
Exposures Patients were assessed by ambulance nurses with positive the face-arm-speech-time test or other stroke suspicion and were evaluated for moderate-to-severe hemiparesis (≥2 National Institutes of Health stroke scale points each on the ipsilateral arm and leg [A2L2 test]). If present, the comprehensive stroke center (CSC) stroke physician was teleconsulted by phone for confirmation of stroke suspicion, assessment of EVT eligibility, and direction to CSC or the nearest primary stroke center. If absent, the nearest hospital was prenotified.
Main Outcomes and Measures Primary outcome: LAO stroke. Secondary outcomes: EVT initiation, onset-to-puncture time, and ONT. Predictive performance measures included sensitivity, specificity, positive and negative predictive values, the overall accuracy for LAO stroke, and EVT initiation.
Results We recorded 2905 patients with code-stroke transports (1420 women [49%]), and of these, 323 (11%) had A2L2+ teleconsultation positive results and were triaged for direct transport to CSC (median age, 73 years [interquartile range (IQR), 64-82 years]; 55 women [48%]). Accuracy for LAO stroke was 87% (positive predictive value, 41%; negative predictive value, 93%) and 91% for EVT initiation (positive predictive value, 26%; negative predictive value, 99%). Endovascular thrombectomy was performed for 84 of 323 patients (26%) with triage-positive results and 35 of 2582 patients (1.4%) with triage-negative results. In EVT cases with a known onset time (77 [3%]), the median OPT was 137 minutes (IQR, 118-180; previous year, 206 minutes [IQR, 160-280]; n = 75) (P < .001). The regional median ONT (337 [12%]) was unchanged at 115 minutes (IQR, 83-164; previous year, 115 minutes [IQR, 85-161]; n = 360) (P = .79). The median CSC IVT door-to-needle time was 13 minutes (IQR, 10-18; 116 [4%]) (previous year, 31 minutes [IQR, 19-38]; n = 45) (P < .001).
Conclusions and Relevance The Stockholm Stroke Triage System, which combines symptom severity and teleconsultation, results in markedly faster EVT delivery without delaying IVT.
中文翻译:
在斯德哥尔摩中风分诊研究中使用症状严重性和远程咨询进行院前中风分诊系统的实施。
重要性 据我们所知,结合症状严重程度和远程会诊的院前中风分诊系统能否准确选择患者进行原发性中风分流并加速分娩血管内血栓切除术(EVT)而不会延迟静脉溶栓治疗(IVT)。
目的 评估新实施的斯德哥尔摩卒中分类系统(SSTS)对大动脉闭塞(LAO)卒中和EVT启动的预测性能。次要目标包括评估Stockholm Stroke Triage System是否缩短了EVT的穿刺开始时间和IVT的穿刺开始时间(ONT)。
设计,地点和参与者 这项基于人群的前瞻性队列研究于2017年10月至2018年10月在斯德哥尔摩地区(瑞典)进行,研究对象包括因急诊中风而被急诊急救车运送到医院的患者(疑似中风)救护车护士和历史控制人员(2016年10月至2017年10月)。排除标准为医院中风和直升机或私人交通工具。在2909名合格患者中,有4名(0.14%)拒绝参加。
暴露 情况由救护护士对患者的面部手臂说话时间测试或其他中风怀疑为阳性,并对患者进行中度至重度偏瘫评估(同侧手臂和腿上≥2个美国国家卫生研究院卒中量表评分[ A2L2测试])。如果有,则通过电话远程咨询综合卒中中心(CSC)的卒中医师,以确认卒中可疑,评估EVT资格以及前往CSC或最近的主要卒中中心的方向。如果缺席,则提前通知最近的医院。
主要结果和措施 主要结果:LAO中风。次要结果:EVT启动,穿刺起效时间和ONT。预测性能指标包括敏感性,特异性,阳性和阴性预测值,LAO中风的总体准确性和EVT起始。
结果 我们记录了2905例中风卒中患者(1420名女性[49%]),其中323例(11%)的A2L2 +远程咨询阳性结果,并被分类为直接转运至CSC(中位年龄73岁[四分位间距] (IQR),64-82岁; 55名女性[48%])。LAO中风的准确性为87%(阳性预测值,41%;阴性预测值,93%)和EVT启动的准确度为91%(阳性预测值,26%;阴性预测值,99%)。323例患者中有84例(26%)进行了血管内血栓切除术,2582例患者中有35例(1.4%)进行了分流阴性。在已知起病时间(77 [3%])的EVT病例中,OPT的中位数为137分钟(IQR,118-180;上一年为206分钟[IQR,160-280]; n = 75)(P <.001)。区域中位数ONT(337 [12%])保持不变,为115分钟(IQR,83-164;上一年为115分钟[IQR,85-161]; n = 360)(P = .79)。CSC IVT门对针时间中位数为13分钟(IQR,10-18; 116 [4%])(上一年为31分钟[IQR,19-38]; n = 45)(P <.001) 。
结论与相关性 斯德哥尔摩中风分类系统结合了症状的严重程度和远程会诊,可显着加快EVT的交付速度,而不会延迟IVT。










































 京公网安备 11010802027423号
京公网安备 11010802027423号