Gastroenterology ( IF 25.7 ) Pub Date : 2020-04-01 , DOI: 10.1053/j.gastro.2020.03.051 Marco Spadaccini 1 , Eduardo Albéniz 2 , Heiko Pohl 3 , Roberta Maselli 4 , Viveksandeep Thoguluva Chandrasekar 5 , Loredana Correale 4 , Andrea Anderloni 4 , Silvia Carrara 4 , Alessandro Fugazza 4 , Matteo Badalamenti 6 , Mineo Iwatate 7 , Giulio Antonelli 8 , Mónica Enguita-Germán 2 , Marco Antonio Álvarez 9 , Prateek Sharma 5 , Douglas K Rex 10 , Cesare Hassan 8 , Alessandro Repici 1
|
Background & Aims
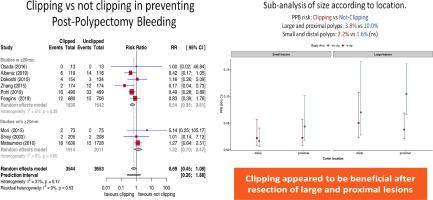
The benefits of prophylactic clipping to prevent bleeding after polypectomy are unclear. We conducted an updated meta-analysis of randomized trials to assess the efficacy of clipping in preventing bleeding after polypectomy, overall and according to polyp size and location.
Methods
We searched the MEDLINE/PubMed, Embase, and Scopus databases for randomized trials that compared the effects of clipping vs not clipping to prevent bleeding after polypectomy. We performed a random-effects meta-analysis to generate pooled relative risks (RRs) with 95% CIs. Multilevel random-effects metaregression analysis was used to combine data on bleeding after polypectomy and estimate associations between rates of bleeding and polyp characteristics.
Results
We analyzed data from 9 trials, comprising 71897 colorectal lesions (22.5% 20 mm or larger; 49.2% with proximal location). Clipping, compared with no clipping, did not significantly reduce the overall risk of postpolypectomy bleeding (2.2% with clipping vs 3.3% with no clipping; RR, 0.69; 95% confidence interval [CI], 0.45–1.08; P = .072). Clipping significantly reduced risk of bleeding after removal of polyps that were 20 mm or larger (4.3% had bleeding after clipping vs 7.6% had bleeding with no clipping; RR, 0.51; 95% CI, 0.33–0.78; P = .020) or that were in a proximal location (3.0% had bleeding after clipping vs 6.2% had bleeding with no clipping; RR, 0.53; 95% CI, 0.35–0.81; P < .001). In multilevel metaregression analysis that adjusted for polyp size and location, prophylactic clipping was significantly associated with reduced risk of bleeding after removal of large proximal polyps (RR, 0.37; 95% CI, 0.22–0.61; P = .021) but not small proximal lesions (RR, 0.88; 95% CI, 0.48–1.62; P = .581).
Conclusions
In a meta-analysis of randomized trials, we found that routine use of prophylactic clipping does not reduce risk of postpolypectomy bleeding overall. However, clipping appeared to reduce bleeding after removal of large (more than 20 mm) proximal lesions.
中文翻译:
大肠内窥镜切除术后的预防性剪裁可防止大的近端息肉出血:随机试验的荟萃分析。
背景与目标
预防性钳夹预防息肉切除术后出血的益处尚不清楚。我们对随机试验进行了更新的荟萃分析,以评估息肉切除术总体上以及根据息肉的大小和位置来预防钳夹预防出血的功效。
方法
我们在MEDLINE / PubMed,Embase和Scopus数据库中进行了随机试验,比较了剪除与不剪除预防息肉切除术后出血的效果。我们进行了一项随机效应荟萃分析,以生成具有95%CI的合并相对风险(RR)。多级随机效应元回归分析用于合并息肉切除术后出血的数据,并估计出血率与息肉特征之间的关联。
结果
我们分析了9个试验的数据,包括71897个结直肠病变(22.5%20 mm或更大;近端位置为49.2%)。与不采用钳夹术相比,采用钳夹术并不能显着降低息肉切除术后出血的总体风险(采用钳夹术的比例为2.2%,不采用钳夹术的比例为3.3%; RR,0.69; 95%可信区间[CI],0.45-1.08;P = .072) 。修剪显着降低了切除20 mm或更大的息肉后出血的风险(4.3%的患者在修剪后有出血,而7.6%的患者没有修剪而有出血; RR,0.51; 95%CI,0.33-0.78;P = .020)或在近端位置(3.0%发生夹闭术后出血,而6.2%发生无夹闭出血; RR,0.53; 95%CI,0.35-0.81;P<.001)。在根据息肉的大小和位置进行了调整的多水平元回归分析中,预防性钳夹与减少大的近端息肉后的出血风险显着相关(RR,0.37; 95%CI,0.22-0.61;P = .021 ),但不小的近端息肉病变(RR,0.88; 95%CI,0.48–1.62;P = .581 )。
结论
在一项随机试验的荟萃分析中,我们发现常规应用预防性钳夹并不能降低息肉切除术后总体出血的风险。但是,在切除较大(大于20 mm)的近端病变后,剪裁似乎可以减少出血。








































 京公网安备 11010802027423号
京公网安备 11010802027423号