JAMA Neurology ( IF 29.0 ) Pub Date : 2020-06-01 , DOI: 10.1001/jamaneurol.2020.0326 Fernando Pico 1, 2, 3 , Bertrand Lapergue 2, 4 , Marc Ferrigno 5, 6 , Charlotte Rosso 7, 8 , Elena Meseguer 9 , Marie-Laure Chadenat 1 , Frederic Bourdain 4 , Michael Obadia 10 , Catherine Hirel 1, 2 , Duc Long Duong 1 , Sandrine Deltour 7 , Philippe Aegerter 11, 12 , Julien Labreuche 13 , Amina Cattenoy 14 , Didier Smadja 15 , Hassan Hosseini 16 , Benoit Guillon 17 , Valérie Wolff 18 , Yves Samson 7 , Charlotte Cordonnier 5, 6 , Pierre Amarenco 3, 9
|
Importance Treatment with remote ischemic perconditioning has been reported to reduce brain infarction volume in animal models of stroke. Whether this neuroprotective effect was observed in patients with acute ischemic stroke remains unknown.
Objective To determine whether treatment with remote ischemic perconditioning administered to the leg of patients with acute ischemic stroke can reduce brain infarction volume growth.
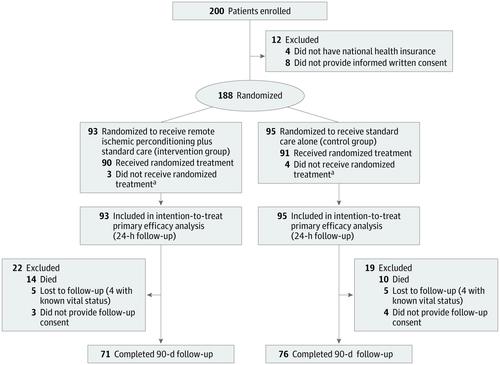
Design, Setting, and Participants This proof-of-concept multicenter prospective randomized open-label with blinded end point clinical trial was performed from January 12, 2015, to May 2, 2018. Patients were recruited from 11 stroke centers in France. Of the 188 patients who received magnetic resonance imaging within 6 hours of symptom onset and were confirmed to have carotid ischemic stroke, 93 were randomized to receive treatment with lower-limb remote ischemic perconditioning in addition to standard care (the intervention group), and 95 were randomized to receive standard care alone (the control group).
Interventions Randomization on a 1:1 ratio to receive treatment with remote ischemic perconditioning (4 cycles of 5-minute inflations and 5-minute deflations to the thigh to 110 mm Hg above systolic blood pressure) in addition to standard care or standard care alone.
Main Outcomes and Measures The change in brain infarction volume growth between baseline and 24 hours, measured by a diffusion-weighted sequence of magnetic resonance imaging scans of the brain.
Results A total of 188 patients (mean [SD] age, 67.2 [15.7] years; 98 men [52.1%]) were included in this intention-to-treat analysis. At hospital admission, the median National Institutes of Health Stroke Scale score was 10 (interquartile range [IQR], 6-16) and the median brain infarction volume was 11.4 cm3 (IQR, 3.6-35.8 cm3); 164 patients (87.2%) received intravenous thrombolysis, and 64 patients (34.0%) underwent mechanical thrombectomy. The median increase in brain infarction growth was 0.30 cm3 (IQR, 0.11-0.48 cm3) in the intervention group and 0.37 cm3 (IQR, 0.19-0.55 cm3) in the control group (mean between-group difference on loge-transformed change, –0.07; 95% CI, –0.33 to 0.18; P = .57). An excellent outcome (defined as a score of 0-1 on the 90-day modified Rankin Scale or a score equal to the prestroke modified Rankin Scale score) was observed in 46 of 90 patients (51.1%) in the intervention group and 37 of 91 patients (40.7%) in the control group (P = .12). No significant differences in 90-day mortality were observed between the intervention and control groups (14 of 90 patients; Kaplan-Meier estimate, 15.8% vs 10 of 91 patients; Kaplan-Meier estimate, 10.4%, respectively; P = .45) or with symptomatic intracerebral hemorrhage (4 of 88 patients [4.5%] in both groups; P = .97).
Conclusions and Relevance In this study, treatment with remote ischemic perconditioning, during or after reperfusion therapies, had no significant effect on brain infarction volume growth at 24 hours after symptom onset.
Trial Registration ClinicalTrials.gov Identifier: NCT02189928
中文翻译:
院内远程缺血性适应对急性缺血性卒中患者脑梗死生长和临床结果的影响:RESCUE BRAIN随机临床试验。
重视 治疗远端缺血perconditioning据报道,以减少中风的动物模型脑梗死容积。在急性缺血性中风患者中是否观察到这种神经保护作用尚不清楚。
目的 探讨急性缺血性脑卒中患者的腿部进行远程缺血性灌注治疗是否可以减少脑梗死体积的增长。
设计,设置和参与者 这项概念验证的多中心前瞻性随机开放标签,盲点临床试验于2015年1月12日至2018年5月2日进行。患者来自法国的11个卒中中心。在188例症状发作6小时内接受磁共振成像并被证实患有颈动脉缺血性卒中的患者中,有93例被随机分配接受除标准护理之外的下肢远程缺血性适应症治疗(干预组),还有95例被随机分配接受标准护理(对照组)。
干预措施 除了标准护理或标准护理外,以1:1的比例随机分配以接受远程缺血性适应治疗(4个周期的5分钟充气和5分钟放气至大腿,收缩压以上110毫米汞柱)。
主要结果和衡量指标: 通过脑部磁共振成像扫描的扩散加权序列来衡量基线和24小时之间脑梗死体积增长的变化。
结果 该意向性治疗分析共纳入188例患者(平均[SD]年龄,67.2 [15.7]岁; 98例男性[52.1%])。入院时,美国国立卫生研究院卒中量表评分中位数为10(四分位间距[IQR],6-16),脑梗死中位数为11.4 cm 3(IQR,3.6-35.8 cm 3);164例患者(87.2%)接受了静脉溶栓治疗,64例患者(34.0%)进行了机械血栓切除术。干预组脑梗死生长的中位数增加为0.30 cm 3(IQR,0.11-0.48 cm 3),对照组为0.37 cm 3(IQR,0.19-0.55 cm 3)(log e的平均组间差异)-转换后的变化–0.07;95%CI,-0.33至0.18;P = .57)。在干预组的90例患者中有46例(51.1%)观察到了极好的结果(定义为90天改良的Rankin量表的0-1得分或等于中风前改良的Rankin量表的得分)。对照组91例(40.7%)(P = 0.12)。干预组和对照组之间的90天死亡率没有显着差异(90名患者中的14名; Kaplan-Meier估计为15.8%,而91名患者中的10名; Kaplan-Meier估计分别为10.4%;P = .45)或伴有症状性脑出血(两组88例中有4例[4.5%];P = 0.97)。
结论与相关性 在这项研究中,在再灌注治疗期间或之后,进行远程缺血性过调治疗,对症状发作后24小时的脑梗死体积增长没有明显影响。
试验注册 ClinicalTrials.gov标识符:NCT02189928


























 京公网安备 11010802027423号
京公网安备 11010802027423号