Gastroenterology ( IF 25.7 ) Pub Date : 2020-03-12 , DOI: 10.1053/j.gastro.2020.03.014 Heiko Pohl 1 , Ian S Grimm 2 , Matthew T Moyer 3 , Muhammad K Hasan 4 , Douglas Pleskow 5 , B Joseph Elmunzer 6 , Mouen A Khashab 7 , Omid Sanaei 7 , Firas H Al-Kawas 8 , Stuart R Gordon 9 , Abraham Mathew 3 , John M Levenick 3 , Harry R Aslanian 10 , Fadi Antaki 11 , Daniel von Renteln 12 , Seth D Crockett 2 , Amit Rastogi 13 , Jeffrey A Gill 14 , Ryan J Law 15 , Pooja A Elias 6 , Maria Pellise 16 , Todd A Mackenzie 17 , Douglas K Rex 18
|
Background & Aims
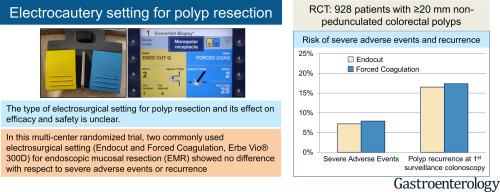
There is debate over the type of electrosurgical setting that should be used for polyp resection. Some endoscopists use a type of blended current (yellow), whereas others prefer coagulation (blue). We performed a single-blinded, randomized trial to determine whether type of electrosurgical setting affects risk of adverse events or recurrence.
Methods
Patients undergoing endoscopic mucosal resection of nonpedunculated colorectal polyps 20 mm or larger (n = 928) were randomly assigned, in a 2 × 2 design, to groups that received clip closure or no clip closure of the resection defect (primary intervention) and then to either a blended current (Endocut Q) or coagulation current (forced coagulation) (Erbe Inc) (secondary intervention and focus of the study). The study was performed at multiple centers, from April 2013 through October 2017. Patients were evaluated 30 days after the procedure (n = 919), and 675 patients underwent a surveillance colonoscopy at a median of 6 months after the procedure. The primary outcome was any severe adverse event in a per patient analysis. Secondary outcomes were complete resection and recurrence at first surveillance colonoscopy in a per polyp analysis.
Results
Serious adverse events occurred in 7.2% of patients in the Endocut group and 7.9% of patients in the forced coagulation group, with no significant differences in the occurrence of types of events. There were no significant differences between groups in proportions of polyps that were completely removed (96% in the Endocut group vs 95% in the forced coagulation group) or the proportion of polyps found to have recurred at surveillance colonoscopy (17% and 17%, respectively). Procedural characteristics were comparable, except that 17% of patients in the Endocut group had immediate bleeding that required an intervention, compared with 11% in the forced coagulation group (P = .006).
Conclusions
In a randomized trial to compare 2 commonly used electrosurgical settings for the resection of large colorectal polyps (Endocut vs forced coagulation), we found no difference in risk of serious adverse events, complete resection rate, or polyp recurrence. Electrosurgical settings can therefore be selected based on endoscopist expertise and preference. Clinicaltrials.gov ID NCT01936948.
中文翻译:
大型随机试验中混合(黄色)与强制凝固(蓝色)电流对不良事件、完全切除或息肉切除术后息肉复发的影响。
背景与目标
关于应该用于息肉切除术的电外科设置类型存在争议。一些内窥镜医师使用一种混合电流(黄色),而其他人则更喜欢凝固(蓝色)。我们进行了一项单盲、随机试验,以确定电外科设置的类型是否会影响不良事件或复发的风险。
方法
接受内窥镜黏膜切除术对 20 mm 或更大的无蒂结直肠息肉(n = 928)的患者以 2 × 2 设计随机分配到接受夹闭或未夹闭切除缺损的组(主要干预),然后进行混合电流(Endocut Q)或凝固电流(强制凝固)(Erbe Inc)(二次干预和研究重点)。该研究于 2013 年 4 月至 2017 年 10 月在多个中心进行。患者在手术后 30 天(n = 919)接受评估,675 名患者在手术后中位时间为 6 个月时接受了监测结肠镜检查。主要结果是每名患者分析中的任何严重不良事件。次要结果是在每个息肉分析中第一次监测结肠镜检查时完全切除和复发。
结果
Endocut 组 7.2% 的患者和强制凝血组 7.9% 的患者发生严重不良事件,事件类型的发生率无显着差异。在完全切除息肉的比例(Endocut 组为 96% 对强制凝固组为 95%)或在监测结肠镜检查中发现的息肉比例(17% 和 17%,分别)。除了 Endocut 组 17% 的患者出现需要干预的立即出血外,程序特征具有可比性,而强制凝血组中的这一比例为 11% ( P = .006)。
结论
在一项比较 2 种常用电外科切除大结直肠息肉的随机试验中(Endocut 与强制凝固术),我们发现严重不良事件的风险、完全切除率或息肉复发没有差异。因此,可以根据内窥镜专家的专业知识和偏好选择电外科设置。Clinicaltrials.gov ID NCT01936948。










































 京公网安备 11010802027423号
京公网安备 11010802027423号