当前位置:
X-MOL 学术
›
J. Am. Coll. Cardiol.
›
论文详情
Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
Tricuspid Intervention Following Pulmonary Valve Replacement in Adults With Congenital Heart Disease
Journal of the American College of Cardiology ( IF 24.0 ) Pub Date : 2020-03-01 , DOI: 10.1016/j.jacc.2019.12.053 Catherine Deshaies , Helen Trottier , Paul Khairy , Mohammed Al-Aklabi , Luc Beauchesne , Pierre-Luc Bernier , Santokh Dhillon , Sanjiv K. Gandhi , Christoph Haller , Camille L. Hancock Friesen , Edward J. Hickey , David Horne , Frédéric Jacques , Marla C. Kiess , Jean Perron , Maria Rodriguez , Nancy C. Poirier
Journal of the American College of Cardiology ( IF 24.0 ) Pub Date : 2020-03-01 , DOI: 10.1016/j.jacc.2019.12.053 Catherine Deshaies , Helen Trottier , Paul Khairy , Mohammed Al-Aklabi , Luc Beauchesne , Pierre-Luc Bernier , Santokh Dhillon , Sanjiv K. Gandhi , Christoph Haller , Camille L. Hancock Friesen , Edward J. Hickey , David Horne , Frédéric Jacques , Marla C. Kiess , Jean Perron , Maria Rodriguez , Nancy C. Poirier
|
BACKGROUND
Tricuspid regurgitation (TR) is common among adults with corrected tetralogy of Fallot (TOF) or pulmonary stenosis (PS) referred for pulmonary valve replacement (PVR). Yet, combined valve surgery remains controversial. OBJECTIVES
This study sought to evaluate the impact of concomitant tricuspid valve intervention (TVI) on post-operative TR, length of hospital stay, and on a composite endpoint consisting of 7 early adverse events (death, reintervention, cardiac electronic device implantation, infection, thromboembolic event, hemodialysis, and readmission). METHODS
The national Canadian cohort enrolled 542 patients with TOF or PS and mild to severe TR who underwent isolated PVR (66.8%) or PVR+TVI (33.2%). Outcomes were abstracted from charts and compared between groups using multivariable logistic and negative binomial regression. RESULTS
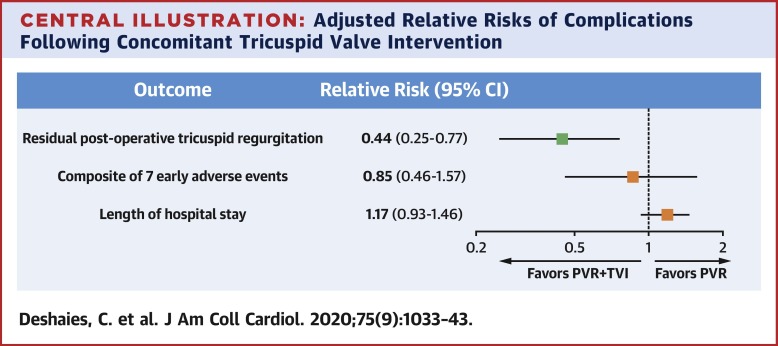
Median age at reintervention was 35.3 years. Regardless of surgery type, TR decreased by at least 1 echocardiographic grade in 35.4%, 66.9%, and 92.8% of patients with pre-operative mild, moderate, and severe insufficiency. In multivariable analyses, PVR+TVI was associated with an additional 2.3-fold reduction in TR grade (odds ratio [OR]: 0.44; 95% confidence interval [CI]: 0.25 to 0.77) without an increase in early adverse events (OR: 0.85; 95% CI: 0.46 to 1.57) or hospitalization time (incidence rate ratio: 1.17; 95% CI: 0.93 to 1.46). Pre-operative TR severity and presence of transvalvular leads independently predicted post-operative TR. In contrast, early adverse events were strongly associated with atrial tachyarrhythmia, extracardiac arteriopathy, and a high body mass index. CONCLUSIONS
In patients with TOF or PS and significant TR, concomitant TVI is safe and results in better early tricuspid valve competence than isolated PVR.
中文翻译:

先天性心脏病成人肺动脉瓣置换术后的三尖瓣干预
背景 三尖瓣关闭不全 (TR) 在矫正法洛四联症 (TOF) 或肺动脉狭窄 (PS) 的成年人中很常见,需要进行肺动脉瓣置换术 (PVR)。然而,联合瓣膜手术仍然存在争议。目的 本研究旨在评估伴随三尖瓣干预 (TVI) 对术后 TR、住院时间以及由 7 个早期不良事件(死亡、再干预、心脏电子设备植入、感染、血栓栓塞事件、血液透析和再入院)。方法 加拿大全国队列招募了 542 名接受孤立 PVR (66.8%) 或 PVR+TVI (33.2%) 的 TOF 或 PS 和轻度至重度 TR 患者。结果从图表中提取出来,并使用多变量逻辑回归和负二项式回归进行组间比较。结果 再次干预的中位年龄为 35.3 岁。无论手术类型如何,术前轻度、中度和重度功能不全的患者中,35.4%、66.9% 和 92.8% 的 TR 降低至少 1 个超声心动图分级。在多变量分析中,PVR+TVI 与 TR 等级额外降低 2.3 倍(优势比 [OR]:0.44;95% 置信区间 [CI]:0.25 至 0.77)相关,而早期不良事件(OR: 0.85;95% CI:0.46 至 1.57)或住院时间(发病率比:1.17;95% CI:0.93 至 1.46)。术前 TR 严重程度和存在跨瓣导联可独立预测术后 TR。相比之下,早期不良事件与房性快速性心律失常、心外动脉病变和高体重指数密切相关。结论 在 TOF 或 PS 和显着 TR 的患者中,
更新日期:2020-03-01
中文翻译:
先天性心脏病成人肺动脉瓣置换术后的三尖瓣干预
背景 三尖瓣关闭不全 (TR) 在矫正法洛四联症 (TOF) 或肺动脉狭窄 (PS) 的成年人中很常见,需要进行肺动脉瓣置换术 (PVR)。然而,联合瓣膜手术仍然存在争议。目的 本研究旨在评估伴随三尖瓣干预 (TVI) 对术后 TR、住院时间以及由 7 个早期不良事件(死亡、再干预、心脏电子设备植入、感染、血栓栓塞事件、血液透析和再入院)。方法 加拿大全国队列招募了 542 名接受孤立 PVR (66.8%) 或 PVR+TVI (33.2%) 的 TOF 或 PS 和轻度至重度 TR 患者。结果从图表中提取出来,并使用多变量逻辑回归和负二项式回归进行组间比较。结果 再次干预的中位年龄为 35.3 岁。无论手术类型如何,术前轻度、中度和重度功能不全的患者中,35.4%、66.9% 和 92.8% 的 TR 降低至少 1 个超声心动图分级。在多变量分析中,PVR+TVI 与 TR 等级额外降低 2.3 倍(优势比 [OR]:0.44;95% 置信区间 [CI]:0.25 至 0.77)相关,而早期不良事件(OR: 0.85;95% CI:0.46 至 1.57)或住院时间(发病率比:1.17;95% CI:0.93 至 1.46)。术前 TR 严重程度和存在跨瓣导联可独立预测术后 TR。相比之下,早期不良事件与房性快速性心律失常、心外动脉病变和高体重指数密切相关。结论 在 TOF 或 PS 和显着 TR 的患者中,


























 京公网安备 11010802027423号
京公网安备 11010802027423号