当前位置:
X-MOL 学术
›
Kidney Int.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Long-term outcomes and response to treatment in diacylglycerol kinase epsilon nephropathy.
Kidney International ( IF 14.8 ) Pub Date : 2020-02-28 , DOI: 10.1016/j.kint.2020.01.045 Vicky Brocklebank 1 , Gurinder Kumar 2 , Alexander J Howie 3 , Jayanthi Chandar 4 , David V Milford 3 , Janet Craze 5 , Jonathan Evans 6 , Eric Finlay 7 , Michael Freundlich 4 , Daniel P Gale 8 , Carol Inward 9 , Martin Mraz 9 , Caroline Jones 10 , William Wong 11 , Stephen D Marks 12 , John Connolly 13 , Bronte M Corner 14 , Kate Smith-Jackson 1 , Patrick R Walsh 1 , Kevin J Marchbank 1 , Claire L Harris 1 , Valerie Wilson 15 , Edwin K S Wong 15 , Michal Malina 16 , Sally Johnson 16 , Neil S Sheerin 1 , David Kavanagh 1
Kidney International ( IF 14.8 ) Pub Date : 2020-02-28 , DOI: 10.1016/j.kint.2020.01.045 Vicky Brocklebank 1 , Gurinder Kumar 2 , Alexander J Howie 3 , Jayanthi Chandar 4 , David V Milford 3 , Janet Craze 5 , Jonathan Evans 6 , Eric Finlay 7 , Michael Freundlich 4 , Daniel P Gale 8 , Carol Inward 9 , Martin Mraz 9 , Caroline Jones 10 , William Wong 11 , Stephen D Marks 12 , John Connolly 13 , Bronte M Corner 14 , Kate Smith-Jackson 1 , Patrick R Walsh 1 , Kevin J Marchbank 1 , Claire L Harris 1 , Valerie Wilson 15 , Edwin K S Wong 15 , Michal Malina 16 , Sally Johnson 16 , Neil S Sheerin 1 , David Kavanagh 1
Affiliation
|
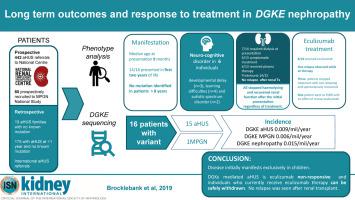
Recessive mutations in diacylglycerol kinase epsilon (DGKE) display genetic pleiotropy, with pathological features reported as either thrombotic microangiopathy or membranoproliferative glomerulonephritis (MPGN), and clinical features of atypical hemolytic uremic syndrome (aHUS), nephrotic syndrome or both. Pathophysiological mechanisms and optimal management strategies have not yet been defined. In prospective and retrospective studies of aHUS referred to the United Kingdom National aHUS service and prospective studies of MPGN referred to the National Registry of Rare Kidney Diseases for MPGN we defined the incidence of DGKE aHUS as 0.009/million/year and so-called DGKE MPGN as 0.006/million/year, giving a combined incidence of 0.015/million/year. Here, we describe a cohort of sixteen individuals with DGKE nephropathy. One presented with isolated nephrotic syndrome. Analysis of pathological features reveals that DGKE mutations give an MPGN-like appearance to different extents, with but more often without changes in arterioles or arteries. In 15 patients presenting with aHUS, ten had concurrent substantial proteinuria. Identified triggering events were rare but coexistent developmental disorders were seen in six. Nine with aHUS experienced at least one relapse, although in only one did a relapse of aHUS occur after age five years. Persistent proteinuria was seen in the majority of cases. Only two individuals have reached end stage renal disease, 20 years after the initial presentation, and in one, renal transplantation was successfully undertaken without relapse. Six individuals received eculizumab. Relapses on treatment occurred in one individual. In four individuals eculizumab was withdrawn, with one spontaneously resolving aHUS relapse occurring. Thus we suggest that DGKE-mediated aHUS is eculizumab non-responsive and that in individuals who currently receive eculizumab therapy it can be safely withdrawn. This has important patient safety and economic implications.
中文翻译:

二酰甘油激酶ε肾病的长期结果和治疗反应。
二酰甘油激酶ε (DGKE) 的隐性突变表现出遗传多效性,其病理特征报告为血栓性微血管病或膜增殖性肾小球肾炎 (MPGN),以及非典型溶血性尿毒症综合征 (aHUS)、肾病综合征或两者兼而有之的临床特征。病理生理机制和最佳管理策略尚未确定。在参考英国国家 aHUS 服务的 aHUS 前瞻性和回顾性研究以及参考国家罕见肾脏病 MPGN 登记处的 MPGN 前瞻性研究中,我们将 DGKE aHUS 的发病率定义为 0.009/百万/年,所谓的 DGKE MPGN为 0.006/百万/年,综合发生率为 0.015/百万/年。在这里,我们描述了一组 16 名 DGKE 肾病患者。一名患者出现孤立性肾病综合征。病理特征分析表明,DGKE 突变在不同程度上呈现 MPGN 样外观,但更常见的是小动脉或动脉没有变化。在 15 名患有 aHUS 的患者中,有 10 名患者同时出现大量蛋白尿。已确定的触发事件很少见,但在六例中发现了共存的发育障碍。 9 名 aHUS 患者至少经历过一次复发,但只有 1 名 aHUS 在五岁后复发。大多数病例出现持续性蛋白尿。在初次发病 20 年后,只有两人达到了终末期肾病,其中一人成功进行了肾移植,没有复发。六人接受了依库珠单抗治疗。一名患者在治疗过程中出现复发。 4 名个体中的依库丽单抗被撤回,其中 1 名个体出现 aHUS 复发自发缓解。 因此,我们建议 DGKE 介导的 aHUS 对依库丽单抗无反应,并且在目前接受依库丽单抗治疗的个体中可以安全地撤回治疗。这具有重要的患者安全和经济影响。
更新日期:2020-02-28
中文翻译:
二酰甘油激酶ε肾病的长期结果和治疗反应。
二酰甘油激酶ε (DGKE) 的隐性突变表现出遗传多效性,其病理特征报告为血栓性微血管病或膜增殖性肾小球肾炎 (MPGN),以及非典型溶血性尿毒症综合征 (aHUS)、肾病综合征或两者兼而有之的临床特征。病理生理机制和最佳管理策略尚未确定。在参考英国国家 aHUS 服务的 aHUS 前瞻性和回顾性研究以及参考国家罕见肾脏病 MPGN 登记处的 MPGN 前瞻性研究中,我们将 DGKE aHUS 的发病率定义为 0.009/百万/年,所谓的 DGKE MPGN为 0.006/百万/年,综合发生率为 0.015/百万/年。在这里,我们描述了一组 16 名 DGKE 肾病患者。一名患者出现孤立性肾病综合征。病理特征分析表明,DGKE 突变在不同程度上呈现 MPGN 样外观,但更常见的是小动脉或动脉没有变化。在 15 名患有 aHUS 的患者中,有 10 名患者同时出现大量蛋白尿。已确定的触发事件很少见,但在六例中发现了共存的发育障碍。 9 名 aHUS 患者至少经历过一次复发,但只有 1 名 aHUS 在五岁后复发。大多数病例出现持续性蛋白尿。在初次发病 20 年后,只有两人达到了终末期肾病,其中一人成功进行了肾移植,没有复发。六人接受了依库珠单抗治疗。一名患者在治疗过程中出现复发。 4 名个体中的依库丽单抗被撤回,其中 1 名个体出现 aHUS 复发自发缓解。 因此,我们建议 DGKE 介导的 aHUS 对依库丽单抗无反应,并且在目前接受依库丽单抗治疗的个体中可以安全地撤回治疗。这具有重要的患者安全和经济影响。










































 京公网安备 11010802027423号
京公网安备 11010802027423号