当前位置:
X-MOL 学术
›
Br. J. Surg.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Minimally invasive oesophagectomy with extended lymph node dissection and thoracic duct resection for early-stage oesophageal squamous cell carcinoma.
British Journal of Surgery ( IF 8.6 ) Pub Date : 2020-02-20 , DOI: 10.1002/bjs.11487 S Matsuda 1 , H Kawakubo 1 , H Takeuchi 2 , M Hayashi 1 , S Mayanagi 1 , R Takemura 3 , T Irino 1 , K Fukuda 1 , R Nakamura 1 , N Wada 1 , Y Kitagawa 1
British Journal of Surgery ( IF 8.6 ) Pub Date : 2020-02-20 , DOI: 10.1002/bjs.11487 S Matsuda 1 , H Kawakubo 1 , H Takeuchi 2 , M Hayashi 1 , S Mayanagi 1 , R Takemura 3 , T Irino 1 , K Fukuda 1 , R Nakamura 1 , N Wada 1 , Y Kitagawa 1
Affiliation
|
BACKGROUND
Oesophageal squamous cell carcinoma is an aggressive disease owing to early and widespread lymph node metastases. Multimodal therapy and radical surgery may improve prognosis. Few studies have investigated the efficacy of radical lymph node and thoracic duct resection.
METHODS
Patients with oesophageal squamous cell carcinoma who underwent transthoracic minimally invasive oesophagectomy (TMIE) for cancer at Keio University Hospital between January 2004 and December 2016 were selected. Between 2004 and 2008, TMIE was performed in the lateral decubitus position without thoracic duct resection (standard TMIE). From 2009 onwards, TMIE with extended lymph node and thoracic duct resection was introduced (extended TMIE). Demographics, co-morbidity, number of retrieved lymph nodes, pathology, postoperative complications and recurrence-free survival (RFS) were compared between groups.
RESULTS
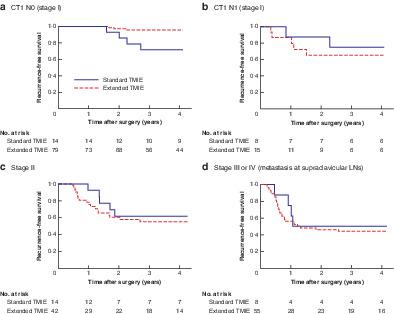
Forty-four patients underwent standard TMIE and 191 extended TMIE. There were no significant differences in clinical and pathological tumour stage or postoperative complications. The extended-TMIE group had more lymph nodes removed at nodal stations 106recL and 112. Among patients with cT1 N0 disease, RFS was better in the extended-TMIE group (P < 0·001), whereas there was no difference in RFS between groups in patients with advanced disease.
CONCLUSION
Extended TMIE including thoracic duct resection increased the number of lymph nodes retrieved and was associated with improved survival in patients with cT1 N0 oesophageal squamous cell carcinoma.
中文翻译:

早期食管鳞状细胞癌的微创食管切除术,扩大的淋巴结清扫术和胸导管切除术。
背景技术由于早期和广泛的淋巴结转移,食道鳞状细胞癌是一种侵袭性疾病。多模式疗法和根治性手术可改善预后。很少有研究调查根治性淋巴结和胸导管切除术的疗效。方法选择2004年1月至2016年12月在庆应义Hospital大学医院接受经胸微创食道癌切除术(TMIE)治疗的食道鳞状细胞癌患者。在2004年至2008年之间,TMIE手术是在不进行胸导管切除的情况下在外侧卧位进行的(标准TMIE)。从2009年起,引入具有扩大的淋巴结和胸导管切除的TMIE(扩展的TMIE)。人口统计学,合并症,回收的淋巴结数目,病理,比较两组之间的术后并发症和无复发生存率(RFS)。结果44例患者接受了标准TMIE,191例接受了扩展TMIE。临床和病理肿瘤分期或术后并发症无明显差异。扩展TMIE组在节点106recL和112的淋巴结处有更多的淋巴结清除。在cT1 N0疾病患者中,扩展TMIE组的RFS更好(P <0·001),而两组之间的RFS没有差异在患有晚期疾病的患者中。结论包括胸腔管切除术在内的扩展TMIE增加了cT1 N0食管鳞癌患者的淋巴结清扫数量,并提高了其生存率。结果44例患者接受了标准TMIE,191例接受了扩展TMIE。临床和病理肿瘤分期或术后并发症无明显差异。扩展TMIE组在节点106recL和112的淋巴结处有更多的淋巴结清除。在cT1 N0疾病患者中,扩展TMIE组的RFS更好(P <0·001),而两组之间的RFS没有差异在患有晚期疾病的患者中。结论包括胸腔管切除术在内的扩展TMIE可以增加cT1 N0食道鳞状细胞癌患者的淋巴结清扫数量,并提高其生存率。结果44例患者接受了标准TMIE,191例接受了扩展TMIE。临床和病理肿瘤分期或术后并发症无明显差异。扩展TMIE组在节点106recL和112的淋巴结处有更多的淋巴结清除。在cT1 N0疾病患者中,扩展TMIE组的RFS更好(P <0·001),而两组之间的RFS没有差异在患有晚期疾病的患者中。结论包括胸腔管切除术在内的扩展TMIE增加了cT1 N0食管鳞癌患者的淋巴结清扫数量,并提高了其生存率。扩展型TMIE组在节点106recL和112处的淋巴结清除率更高。在cT1 N0疾病患者中,扩展型TMIE组的RFS更好(P <0·001),而各组之间的RFS没有差异在患有晚期疾病的患者中。结论包括胸腔管切除术在内的扩展TMIE增加了cT1 N0食管鳞癌患者的淋巴结清扫数量,并提高了其生存率。扩展TMIE组在节点106recL和112的淋巴结处有更多的淋巴结清除。在cT1 N0疾病患者中,扩展TMIE组的RFS更好(P <0·001),而两组之间的RFS没有差异在患有晚期疾病的患者中。结论包括胸腔管切除术在内的扩展TMIE增加了cT1 N0食管鳞癌患者的淋巴结清扫数量,并提高了其生存率。
更新日期:2020-02-20
中文翻译:
早期食管鳞状细胞癌的微创食管切除术,扩大的淋巴结清扫术和胸导管切除术。
背景技术由于早期和广泛的淋巴结转移,食道鳞状细胞癌是一种侵袭性疾病。多模式疗法和根治性手术可改善预后。很少有研究调查根治性淋巴结和胸导管切除术的疗效。方法选择2004年1月至2016年12月在庆应义Hospital大学医院接受经胸微创食道癌切除术(TMIE)治疗的食道鳞状细胞癌患者。在2004年至2008年之间,TMIE手术是在不进行胸导管切除的情况下在外侧卧位进行的(标准TMIE)。从2009年起,引入具有扩大的淋巴结和胸导管切除的TMIE(扩展的TMIE)。人口统计学,合并症,回收的淋巴结数目,病理,比较两组之间的术后并发症和无复发生存率(RFS)。结果44例患者接受了标准TMIE,191例接受了扩展TMIE。临床和病理肿瘤分期或术后并发症无明显差异。扩展TMIE组在节点106recL和112的淋巴结处有更多的淋巴结清除。在cT1 N0疾病患者中,扩展TMIE组的RFS更好(P <0·001),而两组之间的RFS没有差异在患有晚期疾病的患者中。结论包括胸腔管切除术在内的扩展TMIE增加了cT1 N0食管鳞癌患者的淋巴结清扫数量,并提高了其生存率。结果44例患者接受了标准TMIE,191例接受了扩展TMIE。临床和病理肿瘤分期或术后并发症无明显差异。扩展TMIE组在节点106recL和112的淋巴结处有更多的淋巴结清除。在cT1 N0疾病患者中,扩展TMIE组的RFS更好(P <0·001),而两组之间的RFS没有差异在患有晚期疾病的患者中。结论包括胸腔管切除术在内的扩展TMIE可以增加cT1 N0食道鳞状细胞癌患者的淋巴结清扫数量,并提高其生存率。结果44例患者接受了标准TMIE,191例接受了扩展TMIE。临床和病理肿瘤分期或术后并发症无明显差异。扩展TMIE组在节点106recL和112的淋巴结处有更多的淋巴结清除。在cT1 N0疾病患者中,扩展TMIE组的RFS更好(P <0·001),而两组之间的RFS没有差异在患有晚期疾病的患者中。结论包括胸腔管切除术在内的扩展TMIE增加了cT1 N0食管鳞癌患者的淋巴结清扫数量,并提高了其生存率。扩展型TMIE组在节点106recL和112处的淋巴结清除率更高。在cT1 N0疾病患者中,扩展型TMIE组的RFS更好(P <0·001),而各组之间的RFS没有差异在患有晚期疾病的患者中。结论包括胸腔管切除术在内的扩展TMIE增加了cT1 N0食管鳞癌患者的淋巴结清扫数量,并提高了其生存率。扩展TMIE组在节点106recL和112的淋巴结处有更多的淋巴结清除。在cT1 N0疾病患者中,扩展TMIE组的RFS更好(P <0·001),而两组之间的RFS没有差异在患有晚期疾病的患者中。结论包括胸腔管切除术在内的扩展TMIE增加了cT1 N0食管鳞癌患者的淋巴结清扫数量,并提高了其生存率。










































 京公网安备 11010802027423号
京公网安备 11010802027423号