当前位置:
X-MOL 学术
›
Spinal Cord Ser. Cases
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Two case reports of 'locked spondyloptosis': the most severe traumatic cervical spondyloptosis with locked spinous process and vertebral arch into the spinal canal.
Spinal Cord Series and Cases ( IF 0.7 ) Pub Date : 2020-02-18 , DOI: 10.1038/s41394-020-0259-8 Takeru Tsujimoto 1, 2 , Kota Suda 1 , Satoko Matsumoto Harmon 1 , Miki Komatsu 1 , Masahiko Takahata 2 , Norimasa Iwasaki 2 , Akio Minami 1
Spinal Cord Series and Cases ( IF 0.7 ) Pub Date : 2020-02-18 , DOI: 10.1038/s41394-020-0259-8 Takeru Tsujimoto 1, 2 , Kota Suda 1 , Satoko Matsumoto Harmon 1 , Miki Komatsu 1 , Masahiko Takahata 2 , Norimasa Iwasaki 2 , Akio Minami 1
Affiliation
|
INTRODUCTION
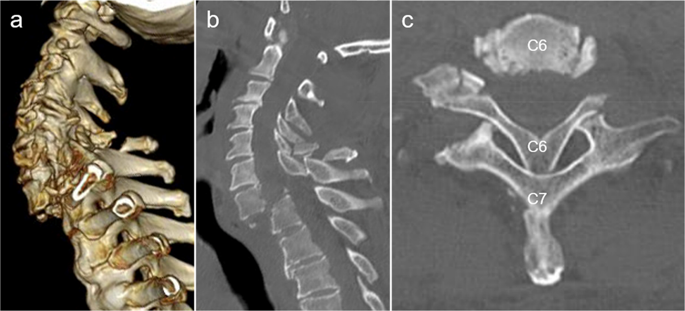
Traumatic cervical spondyloptosis, including compressive-extension stage 5 of Allen's classification of cervical spine injuries, is commonly observed; however, cases involving locked spinous process and vertebral arch into the spinal canal are extremely rare.
CASE PRESENTATION
We present two individuals with spondyloptosis of C7 with locked spinous process of C6 and the vertebral arch into the spinal canal. Closed reduction was unable to be performed due to rigid locking of the cervical spine in the first case, whereas preoperative closed reduction was achieved with mild traction in a prone position after general anaesthesia in the second case. These two individuals underwent spinal fusion via a posterior approach after open or closed reduction. Six months after surgery, both individuals exhibited significant neurological recovery and acquired a stable gait.
DISCUSSION
To the best of our knowledge, this is the first report of traumatic 'locked spondyloptosis' of the spinous process and vertebral arch into the spinal canal. Although high-grade compressive-extension injuries are usually repaired using a combined anterior-posterior approach, repair is possible with a posterior approach alone with reliable anchors, such as pedicle screws or multiple lateral mass screws. Urgent open reduction may be required for locked spondyloptosis when closed reduction is invalid due to rigid locking of the cervical spine.
中文翻译:

“锁定性脊椎下垂”的两个病例报告:最严重的外伤性颈椎下垂,棘突锁定,椎弓进入椎管。
引言 外伤性颈椎下垂,包括 Allen 颈椎损伤分类中的 5 级压缩-伸展性下垂,通常被观察到;然而,涉及锁定棘突和椎弓进入椎管的病例极为罕见。案例介绍 我们介绍了两个 C7 脊椎下垂,C6 棘突锁定,椎弓进入椎管的患者。由于第一种情况下颈椎僵硬,无法进行闭合复位,而第二种情况下,在全麻后在俯卧位轻轻牵引,实现了术前闭合复位。这两个个体在开放或闭合复位后通过后路入路进行了脊柱融合。手术后六个月,两个人都表现出显着的神经功能恢复并获得了稳定的步态。讨论 据我们所知,这是第一份关于棘突和椎弓进入椎管的创伤性“锁定性脊椎下垂”的报告。尽管通常使用前后联合入路修复高级别压缩伸展损伤,但单独使用后入路并使用可靠的锚钉(如椎弓根螺钉或多个侧块螺钉)也可以修复。当颈椎僵硬导致闭合复位无效时,锁定的椎体下垂可能需要紧急开放复位。尽管通常使用前后联合入路修复高级别压缩伸展损伤,但单独使用后入路并使用可靠的锚钉(如椎弓根螺钉或多个侧块螺钉)也可以修复。当由于颈椎僵硬锁定而闭合复位无效时,可能需要紧急切开复位对锁定的脊椎下垂。尽管通常使用前后联合入路修复高级别压缩伸展损伤,但单独使用后入路并使用可靠的锚钉(如椎弓根螺钉或多个侧块螺钉)也可以修复。当由于颈椎僵硬锁定而闭合复位无效时,可能需要紧急切开复位对锁定的脊椎下垂。
更新日期:2020-02-18
中文翻译:
“锁定性脊椎下垂”的两个病例报告:最严重的外伤性颈椎下垂,棘突锁定,椎弓进入椎管。
引言 外伤性颈椎下垂,包括 Allen 颈椎损伤分类中的 5 级压缩-伸展性下垂,通常被观察到;然而,涉及锁定棘突和椎弓进入椎管的病例极为罕见。案例介绍 我们介绍了两个 C7 脊椎下垂,C6 棘突锁定,椎弓进入椎管的患者。由于第一种情况下颈椎僵硬,无法进行闭合复位,而第二种情况下,在全麻后在俯卧位轻轻牵引,实现了术前闭合复位。这两个个体在开放或闭合复位后通过后路入路进行了脊柱融合。手术后六个月,两个人都表现出显着的神经功能恢复并获得了稳定的步态。讨论 据我们所知,这是第一份关于棘突和椎弓进入椎管的创伤性“锁定性脊椎下垂”的报告。尽管通常使用前后联合入路修复高级别压缩伸展损伤,但单独使用后入路并使用可靠的锚钉(如椎弓根螺钉或多个侧块螺钉)也可以修复。当颈椎僵硬导致闭合复位无效时,锁定的椎体下垂可能需要紧急开放复位。尽管通常使用前后联合入路修复高级别压缩伸展损伤,但单独使用后入路并使用可靠的锚钉(如椎弓根螺钉或多个侧块螺钉)也可以修复。当由于颈椎僵硬锁定而闭合复位无效时,可能需要紧急切开复位对锁定的脊椎下垂。尽管通常使用前后联合入路修复高级别压缩伸展损伤,但单独使用后入路并使用可靠的锚钉(如椎弓根螺钉或多个侧块螺钉)也可以修复。当由于颈椎僵硬锁定而闭合复位无效时,可能需要紧急切开复位对锁定的脊椎下垂。










































 京公网安备 11010802027423号
京公网安备 11010802027423号