当前位置:
X-MOL 学术
›
Br. J. Surg.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Recurrence following hemithyroidectomy in patients with low- and intermediate-risk papillary thyroid carcinoma.
British Journal of Surgery ( IF 8.6 ) Pub Date : 2020-02-05 , DOI: 10.1002/bjs.11430 D Ahn 1 , G J Lee 1 , J H Sohn 1
British Journal of Surgery ( IF 8.6 ) Pub Date : 2020-02-05 , DOI: 10.1002/bjs.11430 D Ahn 1 , G J Lee 1 , J H Sohn 1
Affiliation
|
BACKGROUND
This study evaluated the incidence, patterns and risk factors for recurrence after hemithyroidectomy in patients with low- and intermediate-risk papillary thyroid carcinoma (PTC), and verified the predictive role of the risk staging systems in current use.
METHODS
The clinicopathological characteristics and risk categories were analysed according to recurrence in patients who underwent hemithyroidectomy for low- and intermediate-risk conventional PTC, and were followed up for at least 24 months. Five risk staging systems were used to stratify risk: the 2015 American Thyroid Association (ATA) system; Age, Metastases, Extent and Size (AMES) system; Metastases, Age, Complete resection, Invasion and Size (MACIS) system; Grade, Age, Metastases, Extent and Size (GAMES) system; and the eighth AJCC system.
RESULTS
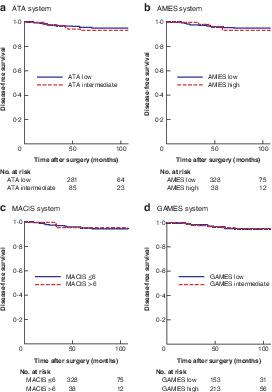
The study included 561 patients; 93·9 per cent of the study population (527 of 561) had a papillary thyroid microcarcinoma 1 cm or smaller in size. At a mean follow-up of 83 months, 25 patients (4·5 per cent) had recurrence; among these patients, 23 (92%) presented with a remaining thyroid lobe. Multifocality was significantly associated with recurrence in univariable and multivariable analyses (adjusted hazard ratio 3·16, 95 per cent c.i. 1·25 to 7·98; P = 0·015). Disease-free survival (DFS) varied according to multifocality (P = 0·010). The five risk staging systems were not associated with recurrence, and their Harrell's C-index ranged from 0·500 to 0·531. DFS rates did not differ between the risk categories in each system.
CONCLUSION
Although the recurrence rate after hemithyroidectomy in patients with low- and intermediate-risk PTC was low, meticulous follow-up focusing on the remaining thyroid lobe is needed for early detection and timely management of recurrence. The risk scoring systems in current use have no predictive role in these patients.
ANTECEDENTES
Este estudio evaluó la incidencia, patrones y factores de riesgo de recidiva tras hemitiroidectomía en pacientes con carcinoma papilar de tiroides (papillary thyroid carcinoma, PTC) de riesgo bajo e intermedio y verificó el papel predictivo de los sistemas de estadificación del riesgo utilizados en la actualidad (risk staging systems, RSSs). MÉTODOS: Se analizaron las características clinicopatológicas y las categorías de riesgo en base a la recidiva en 561 pacientes que fueron sometidos a hemitiroidectomía por PTC convencional de riesgo bajo e intermedio y seguidos durante ≥ 24 meses. Para estratificar el riesgo se utilizaron cinco RSSs, incluyendo el sistema de la American Thyroid Association (ATA) de 2015; la edad, las metástasis, la extensión y el tamaño del sistema AMES; las metástasis, la edad, la resección completa, la invasión y el tamaño del sistema GAMES; y la octava edición de la American Joint Committee on Cancer system (AJCC).
RESULTADOS
La proporción de la población de estudio con microcarcinoma papilar de tiroides de tamaño ≤ 1 cm fue 93,9% (527/561). A los 83 meses de seguimiento, 25 pacientes (4,5%) presentaron recidiva y entre estos pacientes, 23 (92%) no habían sido sometidos a tiroidectomía total. La multifocalidad se asoció significativamente con la recidiva en los análisis univariado y multivariable con un cociente de riesgos instantáneos (hazard ratio, HR) ajustado de 3,163; i.c. del 95% 1,253-7,983; P = 0,015. La supervivencia libre de enfermedad (disease-free survival, DFS) varió según la multifocalidad (P = 0,010). Los cinco RSSs no se asociaron con la recidiva, y su índice C de Harrell fue 0,500-0,531. Las DFSs no fueron diferentes entre las categorías de riesgo de cada RSS. CONCLUSIÓN: La tasa de recidiva tras hemitiroidectomía en pacientes con PTC de riesgo bajo e intermedio fue baja. Sin embargo, es necesario efectuar un seguimiento meticuloso, centrándose en el lóbulo tiroideo restante, para la detección precoz y el tratamiento oportuno de la recidiva. Los RSSs que se utilizan en la actualidad no tienen valor predictivo en estos pacientes.
中文翻译:

中低危甲状腺乳头状癌患者半甲状腺切除术后的复发。
背景本研究评估了低危和中危乳头状甲状腺癌(PTC)患者半甲状腺切除术后复发的发生率,方式和危险因素,并验证了风险分期系统在当前使用中的预测作用。方法根据复发性甲状腺功能低下和中等风险的常规PTC患者的复发情况,分析其临床病理特征和危险类别,并随访至少24个月。五个风险分期系统用于对风险进行分层:2015年美国甲状腺协会(ATA)系统;年龄,转移,范围和大小(AMES)系统;转移,年龄,完全切除,侵袭和大小(MACIS)系统;等级,年龄,转移,范围和大小(GAMES)系统;和第八个AJCC系统。结果该研究包括561例患者。93.9%的研究人群(561个中的527个)患有甲状腺乳头状癌,其大小在1厘米或更小。平均随访83个月,有25例患者(4·5%)复发。在这些患者中,23例(92%)表现出甲状腺叶残留。在单变量和多变量分析中,多焦点与复发密切相关(调整后的危险比为3·16,95%ci为1·25至7·98; P = 0·015)。无病生存期(DFS)因多焦点而异(P = 0·010)。这五个风险分期系统与复发无关,其Harrell的C指数范围为0·500至0·531。在每个系统中,风险类别之间的DFS率没有差异。结论尽管低危和中危PTC患者半甲状腺切除术后的复发率很低,但仍需要针对剩余的甲状腺叶进行细致的随访,以便及早发现和及时治疗复发。当前使用的风险评分系统在这些患者中没有预测作用。评估患癌的先例,光顾了脊柱侧凸癌的原因是乳头状甲状腺癌(乳头状甲状腺癌,PTC),中间是预防性地预防和预防乳糜泻。实际(风险分级系统,RSS)。MÉTODOS:PTC常规检查和常规检查之间的年龄差异≥460,而561例患者的肛门直肠癌就诊。2015年美国甲状腺科协会(ATA)成立的巴西国家广播电视公司RSS;拉埃达(La edad),拉斯梅塔斯塔西斯(lametástasis),拉扩展(exextióny)和塔斯马尼亚(deltamaño)拉斯梅塔斯塔西斯(Lametástasis),拉埃达(la edad),完成记录(reseccióncompleta),入侵(invasióny eltamañodel sistema)游戏;美国癌症系统联合委员会(AJCC)。结果微小癌的癌变原因≤1 cm fue 93,9%(527/561)。损失83人,其中25人(4,5%)的现任法官,23(92%)没有哈比人soid sometidostiroidectomía总数。即时分析的多变量关联性和即时变量的多变量一致性(风险比,HR),准确度为3,163;ic del 95%1,253-7,983;P = 0.015。无疾病生存期(无疾病生存期,DFS),多种疾病(P = 0,010)。Los cinco RSSs no se asociaron con la recidiva,作者Su de nice C de Harrell fue 0,500-0,531。Las DFSs的所有类别RSS不存在。结论:PTC de riesgo bajo e intermedio fue baja的合法身份。禁运罪,不可告人的财产诉讼罪,死刑罪状集中罪,预防犯罪和交通犯罪罪。
更新日期:2020-02-05
中文翻译:
中低危甲状腺乳头状癌患者半甲状腺切除术后的复发。
背景本研究评估了低危和中危乳头状甲状腺癌(PTC)患者半甲状腺切除术后复发的发生率,方式和危险因素,并验证了风险分期系统在当前使用中的预测作用。方法根据复发性甲状腺功能低下和中等风险的常规PTC患者的复发情况,分析其临床病理特征和危险类别,并随访至少24个月。五个风险分期系统用于对风险进行分层:2015年美国甲状腺协会(ATA)系统;年龄,转移,范围和大小(AMES)系统;转移,年龄,完全切除,侵袭和大小(MACIS)系统;等级,年龄,转移,范围和大小(GAMES)系统;和第八个AJCC系统。结果该研究包括561例患者。93.9%的研究人群(561个中的527个)患有甲状腺乳头状癌,其大小在1厘米或更小。平均随访83个月,有25例患者(4·5%)复发。在这些患者中,23例(92%)表现出甲状腺叶残留。在单变量和多变量分析中,多焦点与复发密切相关(调整后的危险比为3·16,95%ci为1·25至7·98; P = 0·015)。无病生存期(DFS)因多焦点而异(P = 0·010)。这五个风险分期系统与复发无关,其Harrell的C指数范围为0·500至0·531。在每个系统中,风险类别之间的DFS率没有差异。结论尽管低危和中危PTC患者半甲状腺切除术后的复发率很低,但仍需要针对剩余的甲状腺叶进行细致的随访,以便及早发现和及时治疗复发。当前使用的风险评分系统在这些患者中没有预测作用。评估患癌的先例,光顾了脊柱侧凸癌的原因是乳头状甲状腺癌(乳头状甲状腺癌,PTC),中间是预防性地预防和预防乳糜泻。实际(风险分级系统,RSS)。MÉTODOS:PTC常规检查和常规检查之间的年龄差异≥460,而561例患者的肛门直肠癌就诊。2015年美国甲状腺科协会(ATA)成立的巴西国家广播电视公司RSS;拉埃达(La edad),拉斯梅塔斯塔西斯(lametástasis),拉扩展(exextióny)和塔斯马尼亚(deltamaño)拉斯梅塔斯塔西斯(Lametástasis),拉埃达(la edad),完成记录(reseccióncompleta),入侵(invasióny eltamañodel sistema)游戏;美国癌症系统联合委员会(AJCC)。结果微小癌的癌变原因≤1 cm fue 93,9%(527/561)。损失83人,其中25人(4,5%)的现任法官,23(92%)没有哈比人soid sometidostiroidectomía总数。即时分析的多变量关联性和即时变量的多变量一致性(风险比,HR),准确度为3,163;ic del 95%1,253-7,983;P = 0.015。无疾病生存期(无疾病生存期,DFS),多种疾病(P = 0,010)。Los cinco RSSs no se asociaron con la recidiva,作者Su de nice C de Harrell fue 0,500-0,531。Las DFSs的所有类别RSS不存在。结论:PTC de riesgo bajo e intermedio fue baja的合法身份。禁运罪,不可告人的财产诉讼罪,死刑罪状集中罪,预防犯罪和交通犯罪罪。










































 京公网安备 11010802027423号
京公网安备 11010802027423号