当前位置:
X-MOL 学术
›
Hypertens. Res.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
The causality between the serum uric acid level and stroke
Hypertension Research ( IF 4.3 ) Pub Date : 2020-01-27 , DOI: 10.1038/s41440-019-0346-z Ryusuke Ae 1 , Mehmet Kanbay 2 , Masanari Kuwabara 3
Hypertension Research ( IF 4.3 ) Pub Date : 2020-01-27 , DOI: 10.1038/s41440-019-0346-z Ryusuke Ae 1 , Mehmet Kanbay 2 , Masanari Kuwabara 3
Affiliation
|
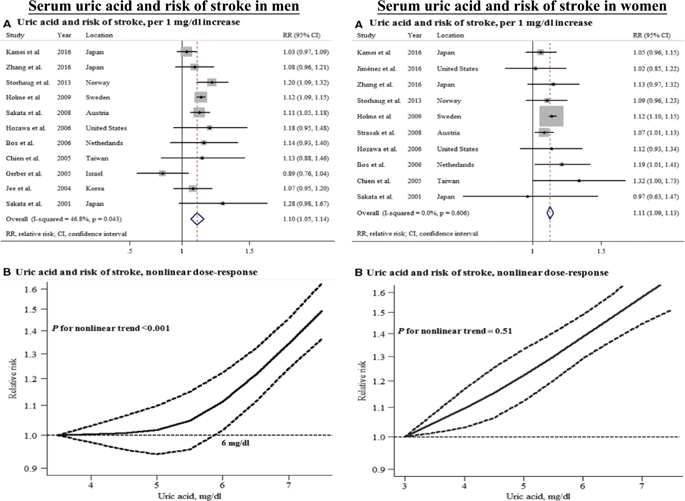
Serum uric acid (SUA) is well known to be associated with cardiovascular risk factors such as hypertension, obesity, metabolic syndrome, dyslipidemia, diabetes mellitus, insulin resistance, chronic kidney disease, etc [1]. However, it is difficult to show the causality between the SUA level and cardiac and cerebrovascular diseases because the former is easily affected by many confounding factors, such as food, alcohol, medication, and so on [1]. For example, a high calorie intake causes obesity and dyslipidemia, as well as hyperuricemia. Obesity and dyslipidemia themselves are known risk factors for cardiac and cerebrovascular diseases, and therefore, we cannot assess whether hyperuricemia itself is a risk factor for cardiac and cerebrovascular diseases. Many epidemiological studies conducted multiple adjustments to reduce the confounding factors, but epidemiological studies do not prove their causality because these adjustments were not able to exclude confounding completely [2]. The causality between SUA and gout is well established, but the causality between SUA and stroke is still to be discussed, as well as that for hypertension [3] or chronic kidney disease [4]. Several meta-analysis studies have indicated that the SUA level is “independently” associated with stroke [5, 6]. Kim S.Y. et al. reported that hyperuricemia was associated with a significantly higher risk of both stroke incidence (relative risk (RR) 1.41) and mortality (RR 1.36) in their metaanalyses of unadjusted study estimates. Moreover, after adjusting for known risk factors such as age, hypertension, diabetes mellitus, and cholesterol, hyperuricemia was significantly associated with both stroke incidence (RR 1.47) and mortality (RR 1.26) [5]. In this meta-analysis, the results did not differ significantly by sex. Another meta-analysis study by Zhong et al. showed similar results: elevated SUA levels were significantly associated with a modestly increased risk of stroke in both men (RR 1.10 per 1 mg/dL increase in SUA) and women (RR 1.11) (Fig. 1) [6]. There seems to be no doubt about the relationship between SUA and stroke. However, some epidemiological studies globally reported inconsistent findings on the relationship between the SUA level and stroke [7–9]; therefore, SUA may not be considered an obvious risk factor for stroke. Even among studies focusing only on a Japanese population, some studies suggested that SUA is an independent predictor of stroke [7, 8], but others reported negative results [9, 10]. These inconsistent findings may be derived from different study settings and participants. Moreover, some studies showed that the relationship between the SUA level and stroke risk differed by sex, indicating a nonlinear (J-shaped) relationship in men, whereas an almost linear trend was observed in women (Fig. 1) [6, 10]. The relationship between the SUA level and stroke is well established, but the causality remains controversial because robust evidence has not been adequately accumulated. The intriguing and timely article by Jiaqi et al. in the present issue of Hypertension Research provided additional evidence of the relationship between the SUA level and stroke [11]. Jiaqi et al. conducted a prospective cohort study using the data from the Circulatory Risk in Communities Study in a general Japanese population, and the results showed that an elevated SUA level is an independent predictor for total and ischemic strokes in women but not in men in a general Japanese population [11]. The strong point of the study is that they conducted multiple adjustments for potential cardiovascular-related factors, not just for age, community, body mass index, smoking and alcohol intake status, systolic blood pressure, atrial fibrillation, serum total cholesterol, triglycerides, estimated glomerular filtration rate, diabetes mellitus, and antihypertensive medication use but also menopausal status in women. Female hormones * Masanari Kuwabara kuwamasa728@gmail.com
中文翻译:

血尿酸水平与中风的因果关系
众所周知,血清尿酸(SUA)与高血压、肥胖、代谢综合征、血脂异常、糖尿病、胰岛素抵抗、慢性肾病等心血管危险因素有关[1]。然而,SUA水平与心脑血管疾病之间的因果关系很难证明,因为前者容易受到许多混杂因素的影响,如食物、酒精、药物等[1]。例如,高热量摄入会导致肥胖和血脂异常,以及高尿酸血症。肥胖和血脂异常本身就是已知的心脑血管疾病的危险因素,因此,我们无法评估高尿酸血症本身是否是心脑血管疾病的危险因素。许多流行病学研究进行了多次调整以减少混杂因素,但流行病学研究并不能证明它们的因果关系,因为这些调整无法完全排除混杂因素 [2]。SUA 与痛风之间的因果关系已明确,但 SUA 与卒中之间的因果关系以及高血压 [3] 或慢性肾病 [4] 之间的因果关系仍有待讨论。几项荟萃分析研究表明,SUA 水平与卒中“独立”相关 [5, 6]。金 SY 等。据报道,在他们对未经调整的研究估计值的荟萃分析中,高尿酸血症与卒中发病率(相对风险(RR)1.41)和死亡率(RR 1.36)显着升高相关。此外,在调整年龄、高血压、糖尿病和胆固醇等已知危险因素后,高尿酸血症与两种卒中发病率均显着相关(RR 1. 47) 和死亡率 (RR 1.26) [5]。在这项荟萃分析中,结果在性别上没有显着差异。钟等人的另一项荟萃分析研究。显示了类似的结果:升高的 SUA 水平与男性(SUA 每增加 1 mg/dL RR 1.10)和女性(RR 1.11)(图 1)的中风风险适度增加显着相关[6]。SUA和中风之间的关系似乎是毫无疑问的。然而,全球一些流行病学研究报告了关于 SUA 水平与卒中之间关系的不一致结果 [7-9];因此,SUA 可能不被认为是中风的明显危险因素。即使在仅针对日本人群的研究中,一些研究表明 SUA 是卒中的独立预测因子 [7, 8],但其他研究报告了阴性结果 [9, 10]。这些不一致的发现可能来自不同的研究环境和参与者。此外,一些研究表明,SUA 水平与中风风险之间的关系因性别而异,表明男性呈非线性(J 形)关系,而女性则观察到几乎呈线性趋势(图 1)[6, 10] . SUA 水平与卒中之间的关系已经确立,但因果关系仍存在争议,因为尚未充分积累强有力的证据。Jiaqi 等人的有趣而及时的文章。在本期《高血压研究》中,为 SUA 水平与中风之间的关系提供了额外的证据 [11]。佳琪等。使用社区循环风险研究的数据在日本一般人群中进行了一项前瞻性队列研究,结果表明,升高的 SUA 水平是女性总卒中和缺血性卒中的独立预测因子,但在日本一般人群中则不是男性 [11]。该研究的优点在于,他们对潜在的心血管相关因素进行了多次调整,而不仅仅是年龄、社区、体重指数、吸烟和饮酒状况、收缩压、心房颤动、血清总胆固醇、甘油三酯、估计肾小球滤过率、糖尿病和抗高血压药物的使用以及女性的更年期状态。女性荷尔蒙 * 桑原正成 kuwamasa728@gmail.com 该研究的优点在于,他们对潜在的心血管相关因素进行了多次调整,而不仅仅是年龄、社区、体重指数、吸烟和饮酒状况、收缩压、心房颤动、血清总胆固醇、甘油三酯、估计肾小球滤过率、糖尿病和抗高血压药物的使用以及女性的更年期状态。女性荷尔蒙 * 桑原正成 kuwamasa728@gmail.com 该研究的优点在于,他们对潜在的心血管相关因素进行了多次调整,而不仅仅是年龄、社区、体重指数、吸烟和饮酒状况、收缩压、心房颤动、血清总胆固醇、甘油三酯、估计肾小球滤过率、糖尿病和抗高血压药物的使用以及女性的更年期状态。女性荷尔蒙 * 桑原正成 kuwamasa728@gmail.com
更新日期:2020-01-27
中文翻译:
血尿酸水平与中风的因果关系
众所周知,血清尿酸(SUA)与高血压、肥胖、代谢综合征、血脂异常、糖尿病、胰岛素抵抗、慢性肾病等心血管危险因素有关[1]。然而,SUA水平与心脑血管疾病之间的因果关系很难证明,因为前者容易受到许多混杂因素的影响,如食物、酒精、药物等[1]。例如,高热量摄入会导致肥胖和血脂异常,以及高尿酸血症。肥胖和血脂异常本身就是已知的心脑血管疾病的危险因素,因此,我们无法评估高尿酸血症本身是否是心脑血管疾病的危险因素。许多流行病学研究进行了多次调整以减少混杂因素,但流行病学研究并不能证明它们的因果关系,因为这些调整无法完全排除混杂因素 [2]。SUA 与痛风之间的因果关系已明确,但 SUA 与卒中之间的因果关系以及高血压 [3] 或慢性肾病 [4] 之间的因果关系仍有待讨论。几项荟萃分析研究表明,SUA 水平与卒中“独立”相关 [5, 6]。金 SY 等。据报道,在他们对未经调整的研究估计值的荟萃分析中,高尿酸血症与卒中发病率(相对风险(RR)1.41)和死亡率(RR 1.36)显着升高相关。此外,在调整年龄、高血压、糖尿病和胆固醇等已知危险因素后,高尿酸血症与两种卒中发病率均显着相关(RR 1. 47) 和死亡率 (RR 1.26) [5]。在这项荟萃分析中,结果在性别上没有显着差异。钟等人的另一项荟萃分析研究。显示了类似的结果:升高的 SUA 水平与男性(SUA 每增加 1 mg/dL RR 1.10)和女性(RR 1.11)(图 1)的中风风险适度增加显着相关[6]。SUA和中风之间的关系似乎是毫无疑问的。然而,全球一些流行病学研究报告了关于 SUA 水平与卒中之间关系的不一致结果 [7-9];因此,SUA 可能不被认为是中风的明显危险因素。即使在仅针对日本人群的研究中,一些研究表明 SUA 是卒中的独立预测因子 [7, 8],但其他研究报告了阴性结果 [9, 10]。这些不一致的发现可能来自不同的研究环境和参与者。此外,一些研究表明,SUA 水平与中风风险之间的关系因性别而异,表明男性呈非线性(J 形)关系,而女性则观察到几乎呈线性趋势(图 1)[6, 10] . SUA 水平与卒中之间的关系已经确立,但因果关系仍存在争议,因为尚未充分积累强有力的证据。Jiaqi 等人的有趣而及时的文章。在本期《高血压研究》中,为 SUA 水平与中风之间的关系提供了额外的证据 [11]。佳琪等。使用社区循环风险研究的数据在日本一般人群中进行了一项前瞻性队列研究,结果表明,升高的 SUA 水平是女性总卒中和缺血性卒中的独立预测因子,但在日本一般人群中则不是男性 [11]。该研究的优点在于,他们对潜在的心血管相关因素进行了多次调整,而不仅仅是年龄、社区、体重指数、吸烟和饮酒状况、收缩压、心房颤动、血清总胆固醇、甘油三酯、估计肾小球滤过率、糖尿病和抗高血压药物的使用以及女性的更年期状态。女性荷尔蒙 * 桑原正成 kuwamasa728@gmail.com 该研究的优点在于,他们对潜在的心血管相关因素进行了多次调整,而不仅仅是年龄、社区、体重指数、吸烟和饮酒状况、收缩压、心房颤动、血清总胆固醇、甘油三酯、估计肾小球滤过率、糖尿病和抗高血压药物的使用以及女性的更年期状态。女性荷尔蒙 * 桑原正成 kuwamasa728@gmail.com 该研究的优点在于,他们对潜在的心血管相关因素进行了多次调整,而不仅仅是年龄、社区、体重指数、吸烟和饮酒状况、收缩压、心房颤动、血清总胆固醇、甘油三酯、估计肾小球滤过率、糖尿病和抗高血压药物的使用以及女性的更年期状态。女性荷尔蒙 * 桑原正成 kuwamasa728@gmail.com










































 京公网安备 11010802027423号
京公网安备 11010802027423号