当前位置:
X-MOL 学术
›
Hypertens. Res.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Glucose-6-phosphate dehydrogenase (G6PD) deficiency is linked with cardiovascular disease
Hypertension Research ( IF 4.3 ) Pub Date : 2020-01-23 , DOI: 10.1038/s41440-020-0402-8 Rajesh Parsanathan 1 , Sushil K Jain 1
Hypertension Research ( IF 4.3 ) Pub Date : 2020-01-23 , DOI: 10.1038/s41440-020-0402-8 Rajesh Parsanathan 1 , Sushil K Jain 1
Affiliation
|
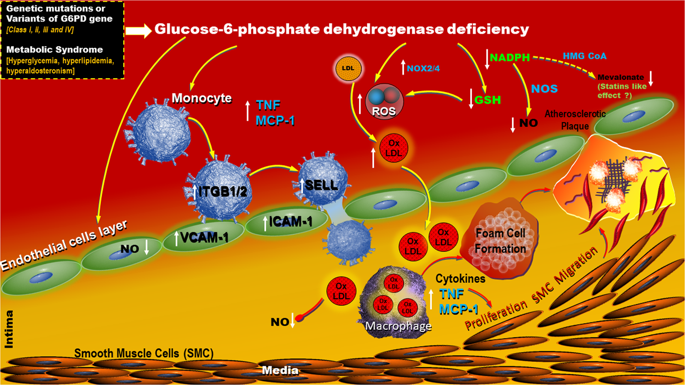
Glucose-6-phosphate dehydrogenase (G6PD) deficiency is the most common diverse X-linked human enzymopathy genetic trait. Males are either G6PD-deficient or normal, but females exhibit a broader range of G6PD deficiency ranging from severe deficiency to normal. An estimated 400 million people are affected by G6PD deficiency globally, and ~160 identified amino acid missense variants cause G6PD deficiency, which is more prevalent in the African continent, Middle East, and South and Southeast Asia. Both male hemizygotes and female homozygotes with G6PD gene deficiency manifest show significantly reduced G6PD enzyme activity, while 80% of female heterozygotes show moderately reduced G6PD enzyme activity. G6PD deficiency risk in females is poorly understood and perhaps often underestimated, and there is a long-standing gender disparity in terms of G6PD deficiency data. In previous studies, G6PD deficiency was investigated in male subjects, but in a recent and exciting cross-sectional study published in Hypertension Research, Zhao et al. [1] showed that 154,917 G6PD-deficient females aged 20–49 had a higher risk of elevated blood pressure and hypertension during prepregnancy and pregnancy periods. In addition, they showed that G6PD deficiency was more obviously associated with systolic blood pressure. Emerging evidence has shown that G6PD deficiency is associated with an increased incidence of CVD among US military personnel and civilians [2, 3]. Recently, a propensity score-matched study performed in a large cohort (9604) in Northern Sardinia, where the population prevalence of G6PD deficiency is the highest in the Mediterranean area, showed a link between G6PD deficiency and the risk of cardiovascular disease (CVD) [4]. Five classifications of G6PD deficiency exist based on enzyme activity levels, as recommended by the WHO. The G6PD A variant is associated with mild to moderate enzyme deficiency (class III) with residual enzyme activity (10–60%) and is found predominately in African Americans (AA). Furthermore, the incidence of G6PD deficiency among AA is 11–14%, compared with only 1% in Caucasians, and AA also show the highest incidence of CVD and a twoto threefold increased risk of stroke compared with other ethnic groups [5]. The high prevalence of hypertension and diabetes in Afro-Caribbeans in the West could be directly related to the incidence of G6PD deficiency in those populations [6]; G6PD deficiency is more severe in AA, as they tend to develop these conditions earlier in life. Impaired redox homeostasis contributes to oxidative stress (OS). G6PD-deficient AA subjects showed elevated levels of OS and decreased levels of glutathione (GSH) [7]. A recent meta-analysis and epidemiological studies have shown that affected individuals can have an increased risk of developing diabetes and CVD [2, 4]. Various G6PD deficiency models have shown the principal role of G6PD deficiency in altering redox homeostasis and the progression of CVD, which predisposes the system to defective vasodilation [6]. In humans, the role of G6PD deficiency and hemolysis has been well documented, and the antioxidant nature of G6PD has underscored its protective effects against the development of a variety of other pathologies, including diabetes and CVD. CVD remains the principal cause of death and disability among patients with diabetes mellitus. Diabetes exacerbates mechanisms underlying atherosclerosis and heart failure. G6PD catalyzes the rate-limiting step in the pentose phosphate pathway, which provides nucleotide precursors for DNA replication as well as cytosolic reducing equivalents of the reduced form of nicotinamide adenine dinucleotide phosphate (NADPH). NADPH contributes to * Sushil K. Jain sjain@lsuhsc.edu
中文翻译:

葡萄糖 6-磷酸脱氢酶 (G6PD) 缺乏与心血管疾病有关
葡萄糖 6-磷酸脱氢酶 (G6PD) 缺乏症是最常见的多种 X 连锁人类酶病遗传特征。男性缺乏 G6PD 或正常,但女性表现出更广泛的 G6PD 缺乏,从严重缺乏到正常。据估计,全球有 4 亿人受到 G6PD 缺乏症的影响,约 160 种已确定的氨基酸错义变异导致 G6PD 缺乏症,这在非洲大陆、中东以及南亚和东南亚更为普遍。G6PD 基因缺陷的男性半合子和女性纯合子均表现出 G6PD 酶活性显着降低,而 80% 的女性杂合子显示 G6PD 酶活性中度降低。女性缺乏 G6PD 的风险知之甚少,而且可能经常被低估,在 G6PD 缺乏数据方面存在长期的性别差异。在之前的研究中,G6PD 缺乏症在男性受试者中进行了研究,但在最近发表在高血压研究中的一项令人兴奋的横断面研究中,赵等人。[1] 表明,154,917 名 20-49 岁的 G6PD 缺陷女性在孕前和怀孕期间血压升高和高血压的风险较高。此外,他们表明 G6PD 缺乏与收缩压更明显相关。新出现的证据表明,G6PD 缺乏与美国军人和平民的 CVD 发病率增加有关 [2, 3]。最近,在撒丁岛北部的一个大型队列 (9604) 中进行了一项倾向评分匹配研究,在地中海地区,G6PD 缺乏症的人群患病率最高,表明 G6PD 缺乏症与心血管疾病 (CVD) 风险之间存在联系[4]。根据世界卫生组织的建议,G6PD 缺乏症存在五种基于酶活性水平的分类。G6PD A 变体与轻度至中度酶缺乏症(III 类)相关,具有残留酶活性(10-60%),主要见于非裔美国人 (AA)。此外,AA 中 G6PD 缺乏的发生率为 11-14%,而白种人仅为 1%,并且与其他种族相比,AA 的 CVD 发生率最高,卒中风险增加 2-3 倍 [5]。西方非裔加勒比地区高血压和糖尿病的高患病率可能与这些人群中 G6PD 缺乏症的发生率直接相关 [6];G6PD 缺乏症在 AA 中更为严重,因为他们倾向于在生命的早期发展这些疾病。氧化还原稳态受损会导致氧化应激 (OS)。G6PD 缺陷型 AA 受试者的 OS 水平升高,谷胱甘肽 (GSH) 水平降低 [7]。最近的一项荟萃分析和流行病学研究表明,受影响的个体患糖尿病和 CVD 的风险会增加 [2, 4]。各种 G6PD 缺乏症模型已显示 G6PD 缺乏症在改变氧化还原稳态和 CVD 进展方面的主要作用,这使系统易于出现血管舒张缺陷 [6]。在人类中,G6PD 缺乏症和溶血的作用已得到充分证明,G6PD 的抗氧化性质强调了其对多种其他疾病发展的保护作用,包括糖尿病和 CVD。心血管疾病仍然是糖尿病患者死亡和残疾的主要原因。糖尿病会加剧动脉粥样硬化和心力衰竭的潜在机制。G6PD 催化磷酸戊糖途径中的限速步骤,为 DNA 复制提供核苷酸前体以及还原形式的烟酰胺腺嘌呤二核苷酸磷酸 (NADPH) 的胞质还原等价物。NADPH 有助于 * Sushil K. Jain sjain@lsuhsc.edu 包括糖尿病和心血管疾病。心血管疾病仍然是糖尿病患者死亡和残疾的主要原因。糖尿病会加剧动脉粥样硬化和心力衰竭的潜在机制。G6PD 催化磷酸戊糖途径中的限速步骤,为 DNA 复制提供核苷酸前体以及还原形式的烟酰胺腺嘌呤二核苷酸磷酸 (NADPH) 的胞质还原等价物。NADPH 有助于 * Sushil K. Jain sjain@lsuhsc.edu 包括糖尿病和心血管疾病。心血管疾病仍然是糖尿病患者死亡和残疾的主要原因。糖尿病会加剧动脉粥样硬化和心力衰竭的潜在机制。G6PD 催化磷酸戊糖途径中的限速步骤,为 DNA 复制提供核苷酸前体以及还原形式的烟酰胺腺嘌呤二核苷酸磷酸 (NADPH) 的胞质还原等价物。NADPH 有助于 * Sushil K. Jain sjain@lsuhsc.edu 它提供了用于 DNA 复制的核苷酸前体以及还原形式的烟酰胺腺嘌呤二核苷酸磷酸 (NADPH) 的胞质还原等价物。NADPH 有助于 * Sushil K. Jain sjain@lsuhsc.edu 它提供了用于 DNA 复制的核苷酸前体以及还原形式的烟酰胺腺嘌呤二核苷酸磷酸 (NADPH) 的胞质还原等价物。NADPH 有助于 * Sushil K. Jain sjain@lsuhsc.edu
更新日期:2020-01-23
中文翻译:
葡萄糖 6-磷酸脱氢酶 (G6PD) 缺乏与心血管疾病有关
葡萄糖 6-磷酸脱氢酶 (G6PD) 缺乏症是最常见的多种 X 连锁人类酶病遗传特征。男性缺乏 G6PD 或正常,但女性表现出更广泛的 G6PD 缺乏,从严重缺乏到正常。据估计,全球有 4 亿人受到 G6PD 缺乏症的影响,约 160 种已确定的氨基酸错义变异导致 G6PD 缺乏症,这在非洲大陆、中东以及南亚和东南亚更为普遍。G6PD 基因缺陷的男性半合子和女性纯合子均表现出 G6PD 酶活性显着降低,而 80% 的女性杂合子显示 G6PD 酶活性中度降低。女性缺乏 G6PD 的风险知之甚少,而且可能经常被低估,在 G6PD 缺乏数据方面存在长期的性别差异。在之前的研究中,G6PD 缺乏症在男性受试者中进行了研究,但在最近发表在高血压研究中的一项令人兴奋的横断面研究中,赵等人。[1] 表明,154,917 名 20-49 岁的 G6PD 缺陷女性在孕前和怀孕期间血压升高和高血压的风险较高。此外,他们表明 G6PD 缺乏与收缩压更明显相关。新出现的证据表明,G6PD 缺乏与美国军人和平民的 CVD 发病率增加有关 [2, 3]。最近,在撒丁岛北部的一个大型队列 (9604) 中进行了一项倾向评分匹配研究,在地中海地区,G6PD 缺乏症的人群患病率最高,表明 G6PD 缺乏症与心血管疾病 (CVD) 风险之间存在联系[4]。根据世界卫生组织的建议,G6PD 缺乏症存在五种基于酶活性水平的分类。G6PD A 变体与轻度至中度酶缺乏症(III 类)相关,具有残留酶活性(10-60%),主要见于非裔美国人 (AA)。此外,AA 中 G6PD 缺乏的发生率为 11-14%,而白种人仅为 1%,并且与其他种族相比,AA 的 CVD 发生率最高,卒中风险增加 2-3 倍 [5]。西方非裔加勒比地区高血压和糖尿病的高患病率可能与这些人群中 G6PD 缺乏症的发生率直接相关 [6];G6PD 缺乏症在 AA 中更为严重,因为他们倾向于在生命的早期发展这些疾病。氧化还原稳态受损会导致氧化应激 (OS)。G6PD 缺陷型 AA 受试者的 OS 水平升高,谷胱甘肽 (GSH) 水平降低 [7]。最近的一项荟萃分析和流行病学研究表明,受影响的个体患糖尿病和 CVD 的风险会增加 [2, 4]。各种 G6PD 缺乏症模型已显示 G6PD 缺乏症在改变氧化还原稳态和 CVD 进展方面的主要作用,这使系统易于出现血管舒张缺陷 [6]。在人类中,G6PD 缺乏症和溶血的作用已得到充分证明,G6PD 的抗氧化性质强调了其对多种其他疾病发展的保护作用,包括糖尿病和 CVD。心血管疾病仍然是糖尿病患者死亡和残疾的主要原因。糖尿病会加剧动脉粥样硬化和心力衰竭的潜在机制。G6PD 催化磷酸戊糖途径中的限速步骤,为 DNA 复制提供核苷酸前体以及还原形式的烟酰胺腺嘌呤二核苷酸磷酸 (NADPH) 的胞质还原等价物。NADPH 有助于 * Sushil K. Jain sjain@lsuhsc.edu 包括糖尿病和心血管疾病。心血管疾病仍然是糖尿病患者死亡和残疾的主要原因。糖尿病会加剧动脉粥样硬化和心力衰竭的潜在机制。G6PD 催化磷酸戊糖途径中的限速步骤,为 DNA 复制提供核苷酸前体以及还原形式的烟酰胺腺嘌呤二核苷酸磷酸 (NADPH) 的胞质还原等价物。NADPH 有助于 * Sushil K. Jain sjain@lsuhsc.edu 包括糖尿病和心血管疾病。心血管疾病仍然是糖尿病患者死亡和残疾的主要原因。糖尿病会加剧动脉粥样硬化和心力衰竭的潜在机制。G6PD 催化磷酸戊糖途径中的限速步骤,为 DNA 复制提供核苷酸前体以及还原形式的烟酰胺腺嘌呤二核苷酸磷酸 (NADPH) 的胞质还原等价物。NADPH 有助于 * Sushil K. Jain sjain@lsuhsc.edu 它提供了用于 DNA 复制的核苷酸前体以及还原形式的烟酰胺腺嘌呤二核苷酸磷酸 (NADPH) 的胞质还原等价物。NADPH 有助于 * Sushil K. Jain sjain@lsuhsc.edu 它提供了用于 DNA 复制的核苷酸前体以及还原形式的烟酰胺腺嘌呤二核苷酸磷酸 (NADPH) 的胞质还原等价物。NADPH 有助于 * Sushil K. Jain sjain@lsuhsc.edu










































 京公网安备 11010802027423号
京公网安备 11010802027423号