当前位置:
X-MOL 学术
›
JAMA Surg.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Effect of Multimodal Prehabilitation vs Postoperative Rehabilitation on 30-Day Postoperative Complications for Frail Patients Undergoing Resection of Colorectal Cancer: A Randomized Clinical Trial.
JAMA Surgery ( IF 15.7 ) Pub Date : 2020-01-22 , DOI: 10.1001/jamasurg.2019.5474 Francesco Carli 1 , Guillaume Bousquet-Dion 1 , Rashami Awasthi 1 , Noha Elsherbini 2 , Sender Liberman 3 , Marylise Boutros 4 , Barry Stein 3 , Patrick Charlebois 3 , Gabriela Ghitulescu 4 , Nancy Morin 4 , Thomas Jagoe 5 , Celena Scheede-Bergdahl 6 , Enrico Maria Minnella 1 , Julio F Fiore 3
JAMA Surgery ( IF 15.7 ) Pub Date : 2020-01-22 , DOI: 10.1001/jamasurg.2019.5474 Francesco Carli 1 , Guillaume Bousquet-Dion 1 , Rashami Awasthi 1 , Noha Elsherbini 2 , Sender Liberman 3 , Marylise Boutros 4 , Barry Stein 3 , Patrick Charlebois 3 , Gabriela Ghitulescu 4 , Nancy Morin 4 , Thomas Jagoe 5 , Celena Scheede-Bergdahl 6 , Enrico Maria Minnella 1 , Julio F Fiore 3
Affiliation
|
Importance
Research supports use of prehabilitation to optimize physical status before and after colorectal cancer resection, but its effect on postoperative complications remains unclear. Frail patients are a target for prehabilitation interventions owing to increased risk for poor postoperative outcomes.
Objective
To assess the extent to which a prehabilitation program affects 30-day postoperative complications in frail patients undergoing colorectal cancer resection compared with postoperative rehabilitation.
Design, Setting, and Participants
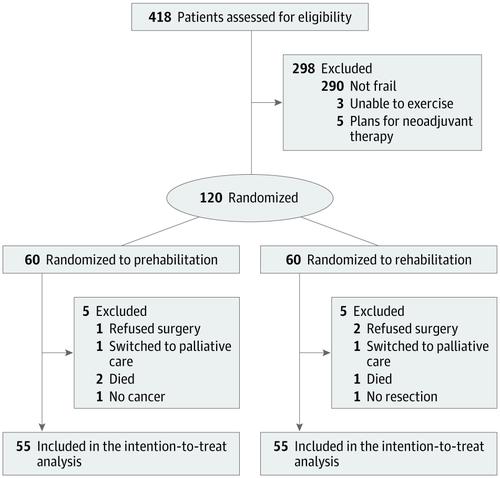
This single-blind, parallel-arm, superiority randomized clinical trial recruited patients undergoing colorectal cancer resection from September 7, 2015, through June 19, 2019. Patients were followed up for 4 weeks before surgery and 4 weeks after surgery at 2 university-affiliated tertiary hospitals. A total of 418 patients 65 years or older were assessed for eligibility. Of these, 298 patients were excluded (not frail [n = 290], unable to exercise [n = 3], and planned neoadjuvant treatment [n = 5]), and 120 frail patients (Fried Frailty Index,≥2) were randomized. Ten patients were excluded after randomization because they refused surgery (n = 3), died before surgery (n = 3), had no cancer (n = 1), had surgery without bowel resection (n = 1), or were switched to palliative care (n = 2). Hence, 110 patients were included in the intention-to-treat analysis (55 in the prehabilitation [Prehab] and 55 in the rehabilitation [Rehab] groups). Data were analyzed from July 25 through August 21, 2019.
Interventions
Multimodal program involving exercise, nutritional, and psychological interventions initiated before (Prehab group) or after (Rehab group) surgery. All patients were treated within a standardized enhanced recovery pathway.
Main Outcomes and Measures
The primary outcome included the Comprehensive Complications Index measured at 30 days after surgery. Secondary outcomes were 30-day overall and severe complications, primary and total length of hospital stay, 30-day emergency department visits and hospital readmissions, recovery of walking capacity, and patient-reported outcome measures.
Results
Of 110 patients randomized, mean (SD) age was 78 (7) years; 52 (47.3%) were men and 58 (52.7%) were women; 31 (28.2%) had rectal cancer; and 87 (79.1%) underwent minimally invasive surgery. There was no between-group difference in the primary outcome measure, 30-day Comprehensive Complications Index (adjusted mean difference, -3.2; 95% CI, -11.8 to 5.3; P = .45). Secondary outcome measures were also not different between groups.
Conclusions and Relevance
In frail patients undergoing colorectal cancer resection (predominantly minimally invasive) within an enhanced recovery pathway, a multimodal prehabilitation program did not affect postoperative outcomes. Alternative strategies should be considered to optimize treatment of frail patients preoperatively.
Trial Registration
ClinicalTrials.gov identifier: NCT02502760.
中文翻译:

多模式康复与术后康复对大肠癌切除术后体弱患者术后30天并发症的影响:一项随机临床试验。
重要研究支持大肠癌切除术之前和之后的术前康复,以优化身体状况,但其对术后并发症的影响尚不清楚。体弱的患者由于术后不良预后的风险增加而成为康复前干预的目标。目的评估与手术后康复相比,术前准备计划对大肠癌切除术后体弱患者术后30天并发症的影响程度。设计,设置和参加者这项单盲,平行臂优越性随机临床试验招募了从2015年9月7日至2019年6月19日接受结直肠癌切除术的患者。对患者进行了手术前4周和术后4周的随访。在两家大学附属三级医院进行手术。总共对418名65岁或65岁以上的患者进行了资格评估。其中,排除了298例患者(不虚弱[n = 290],不能运动[n = 3]和计划的新辅助治疗[n = 5]),并随机分配了120例虚弱的患者(Fried Frailty Index,≥2)。 。随机分组后有10名患者被排除在外,因为他们拒绝手术(n = 3),在手术前死亡(n = 3),没有癌症(n = 1),未经肠切除的手术(n = 1)或转为姑息治疗护理(n = 2)。因此,意向性治疗分析包括110名患者(康复前[Rehab]组55名,康复[Rehab]组55名)。分析了从2019年7月25日至2019年8月21日的数据。干预多式联运计划涉及运动,营养,术前(Prehab组)或术后(Rehab组)进行的心理干预。所有患者均在标准化的增强恢复途径中接受治疗。主要结果和措施主要结果包括手术后30天测得的综合并发症指数。次要结局为30天的总体和严重并发症,住院的主要和总时间,急诊科就诊30天和住院再入院,步行能力的恢复以及患者报告的结局指标。结果随机分配的110名患者的平均(SD)年龄为78(7)岁;男性为52(47.3%),女性为58(52.7%);31名(28.2%)患有直肠癌;其中87例(79.1%)接受了微创手术。主要结局指标之间没有组间差异,30天综合并发症指数(调整后的平均差异为-3.2; 95%CI为-11.8至5.3; P = 0.45)。两组之间的次要结局指标也没有差异。结论与相关性在恢复途径增强的情况下接受结直肠癌切除(主要是微创)的体弱患者中,多模式康复计划不会影响术后结果。应考虑采用替代策略以优化术前虚弱患者的治疗。试验注册ClinicalTrials.gov标识符:NCT02502760。多模式康复计划不会影响术后结果。应考虑采用替代策略以优化术前虚弱患者的治疗。试验注册ClinicalTrials.gov标识符:NCT02502760。多模式康复计划不会影响术后结果。应考虑采用替代策略以优化术前虚弱患者的治疗。试验注册ClinicalTrials.gov标识符:NCT02502760。
更新日期:2020-03-19
中文翻译:
多模式康复与术后康复对大肠癌切除术后体弱患者术后30天并发症的影响:一项随机临床试验。
重要研究支持大肠癌切除术之前和之后的术前康复,以优化身体状况,但其对术后并发症的影响尚不清楚。体弱的患者由于术后不良预后的风险增加而成为康复前干预的目标。目的评估与手术后康复相比,术前准备计划对大肠癌切除术后体弱患者术后30天并发症的影响程度。设计,设置和参加者这项单盲,平行臂优越性随机临床试验招募了从2015年9月7日至2019年6月19日接受结直肠癌切除术的患者。对患者进行了手术前4周和术后4周的随访。在两家大学附属三级医院进行手术。总共对418名65岁或65岁以上的患者进行了资格评估。其中,排除了298例患者(不虚弱[n = 290],不能运动[n = 3]和计划的新辅助治疗[n = 5]),并随机分配了120例虚弱的患者(Fried Frailty Index,≥2)。 。随机分组后有10名患者被排除在外,因为他们拒绝手术(n = 3),在手术前死亡(n = 3),没有癌症(n = 1),未经肠切除的手术(n = 1)或转为姑息治疗护理(n = 2)。因此,意向性治疗分析包括110名患者(康复前[Rehab]组55名,康复[Rehab]组55名)。分析了从2019年7月25日至2019年8月21日的数据。干预多式联运计划涉及运动,营养,术前(Prehab组)或术后(Rehab组)进行的心理干预。所有患者均在标准化的增强恢复途径中接受治疗。主要结果和措施主要结果包括手术后30天测得的综合并发症指数。次要结局为30天的总体和严重并发症,住院的主要和总时间,急诊科就诊30天和住院再入院,步行能力的恢复以及患者报告的结局指标。结果随机分配的110名患者的平均(SD)年龄为78(7)岁;男性为52(47.3%),女性为58(52.7%);31名(28.2%)患有直肠癌;其中87例(79.1%)接受了微创手术。主要结局指标之间没有组间差异,30天综合并发症指数(调整后的平均差异为-3.2; 95%CI为-11.8至5.3; P = 0.45)。两组之间的次要结局指标也没有差异。结论与相关性在恢复途径增强的情况下接受结直肠癌切除(主要是微创)的体弱患者中,多模式康复计划不会影响术后结果。应考虑采用替代策略以优化术前虚弱患者的治疗。试验注册ClinicalTrials.gov标识符:NCT02502760。多模式康复计划不会影响术后结果。应考虑采用替代策略以优化术前虚弱患者的治疗。试验注册ClinicalTrials.gov标识符:NCT02502760。多模式康复计划不会影响术后结果。应考虑采用替代策略以优化术前虚弱患者的治疗。试验注册ClinicalTrials.gov标识符:NCT02502760。










































 京公网安备 11010802027423号
京公网安备 11010802027423号