当前位置:
X-MOL 学术
›
Hypertens. Res.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
A case of adrenaline-predominant paraganglioma diagnosed with a state of shock after glucagon injection
Hypertension Research ( IF 4.3 ) Pub Date : 2020-01-22 , DOI: 10.1038/s41440-020-0400-x Hiroshi Nakama 1 , Mitsuhiro Okamoto 1 , Keiko Kurosawa 2 , Hiromitsu Mimata 3 , Tsutom Daa 4 , Kazuhiro Takekoshi 5 , Koro Gotoh 1 , Takayuki Masaki 1 , Hirotaka Shibata 1
Hypertension Research ( IF 4.3 ) Pub Date : 2020-01-22 , DOI: 10.1038/s41440-020-0400-x Hiroshi Nakama 1 , Mitsuhiro Okamoto 1 , Keiko Kurosawa 2 , Hiromitsu Mimata 3 , Tsutom Daa 4 , Kazuhiro Takekoshi 5 , Koro Gotoh 1 , Takayuki Masaki 1 , Hirotaka Shibata 1
Affiliation
|
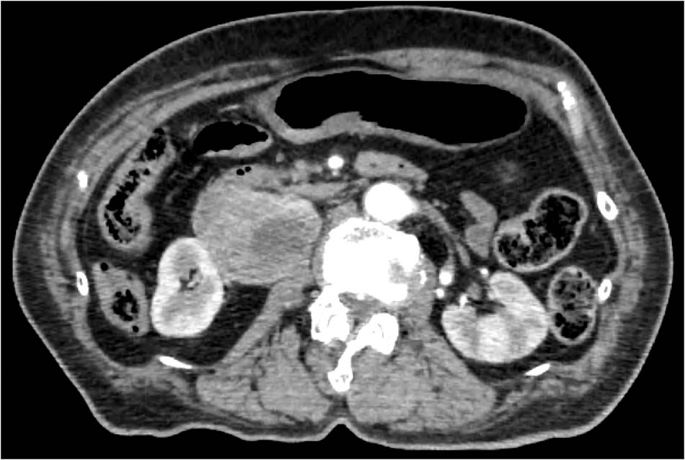
Pheochromocytoma-paraganglioma (PPGL), a catecholaminesecreting tumor, is a rare and curable cause of hypertension, with frequent complications of headache, sweating, palpitation, and hyperhidrosis. PPGL may precipitate hypertensive crisis with several agents, such as contrast medium, glucagon, and metoclopramide. We report a case of a recurrent right retroperitoneal paraganglioma that was diagnosed by hypertensive crisis with glucagon administration for pretreatment for endoscopic examination 17 years after surgery on a right adrenal pheochromocytoma. A 75-year-old woman who had headache, paroxysmal hypertension, and hyperhidrosis for 3 years was diagnosed with a pheochromocytoma from an endocrine profile and computed tomography (CT) scan, which showed a right adrenal tumor in 1999. Approximately 10 years after the surgery, she had paroxysmal hypertension again. In 2016, she was scheduled for gastroscopy. Immediately before the gastroscopy, 1 mg of glucagon was administered to inhibit gastrointestinal motility. Within minutes, she went into shock. The gastroscopy was canceled, and she was transferred to the emergency department of our hospital. On initial examination, imaging at the time of admission included an abdominal CT scan. The enhanced CT scan revealed a defined mass of 62 × 50mm in size at the hilum of the right kidney (Fig. 1). She received a multidisciplinary treatment because of significant hypertension and tachycardia. The blood pressure and the pulse were gradually controlled after intravenous administration of an α-adrenergic blocker, phentolamine. No patient with pheochromocytoma, paraganglioma, or related genetic disease (such as von Hippel-Lindau (VHL) disease) was found in her family history. Considering that right total adrenalectomy had been previously performed, these physiological findings were assumed to be the result of catecholamine crisis derived from an extra-adrenal paraganglioma. Adrenal magnetic resonance imaging (MRI) in T2WI images showed a markedly high intensity and heterogeneous mass of 50 × 56 × 79mm in size at the hilum of the right kidney. The data for urine catecholamine before the right adrenalectomy are listed in Table 1. The hypersecretion of adrenaline as well as noradrenaline, but not dopamine, was confirmed by a 24-h urine test. Impaired glucose tolerance was also observed. The patient underwent I-meta-iodobenzylguandine (I-MIBG)
中文翻译:

注射胰高血糖素后诊断为休克状态的肾上腺素为主的副神经节瘤一例
嗜铬细胞瘤-副神经节瘤 (PPGL) 是一种分泌儿茶酚胺的肿瘤,是一种罕见且可治愈的高血压病因,常伴有头痛、出汗、心悸和多汗症等并发症。PPGL 可能会与几种药物一起引发高血压危象,例如造影剂、胰高血糖素和甲氧氯普胺。我们报告了一例复发性右腹膜后副神经节瘤,在右肾上腺嗜铬细胞瘤手术后 17 年被诊断为高血压危象并给予胰高血糖素进行内镜检查预处理。一名 75 岁女性,患有头痛、阵发性高血压和多汗症 3 年,经内分泌和计算机断层扫描 (CT) 扫描诊断为嗜铬细胞瘤,1999 年显示右侧肾上腺肿瘤。大约 10 年后手术,她又患了阵发性高血压。2016年,她被安排进行胃镜检查。在胃镜检查前立即给予 1 mg 胰高血糖素以抑制胃肠蠕动。几分钟后,她震惊了。胃镜检查取消,转入我院急诊科。在最初的检查中,入院时的成像包括腹部 CT 扫描。增强 CT 扫描显示右肾门部有一个大小为 62 × 50mm 的明确肿块(图 1)。由于明显的高血压和心动过速,她接受了多学科治疗。静脉注射α-肾上腺素能阻滞剂酚妥拉明后,血压和脉搏逐渐得到控制。无嗜铬细胞瘤、副神经节瘤、在她的家族史中发现了或相关的遗传疾病(如 von Hippel-Lindau (VHL) 病)。考虑到之前已经进行了右侧全肾上腺切除术,这些生理学发现被认为是源自肾上腺外副神经节瘤的儿茶酚胺危象的结果。T2WI 图像中的肾上腺磁共振成像 (MRI) 显示右肾门部有明显高强度和不均匀的肿块,大小为 50 × 56 × 79mm。右肾上腺切除术前尿儿茶酚胺的数据列于表 1。肾上腺素和去甲肾上腺素的分泌过多,但不是多巴胺,通过 24 小时尿检证实。还观察到葡萄糖耐量受损。患者接受了 I-间碘苄胍 (I-MIBG) 考虑到之前已经进行了右侧全肾上腺切除术,这些生理学发现被认为是源自肾上腺外副神经节瘤的儿茶酚胺危象的结果。T2WI 图像中的肾上腺磁共振成像 (MRI) 显示右肾门部有明显高强度和不均匀的肿块,大小为 50 × 56 × 79mm。右肾上腺切除术前尿儿茶酚胺的数据列于表 1。肾上腺素和去甲肾上腺素分泌过多,但多巴胺不分泌,通过 24 小时尿检证实。还观察到葡萄糖耐量受损。患者接受了 I-间碘苄胍 (I-MIBG) 考虑到之前已经进行了右侧全肾上腺切除术,这些生理学发现被认为是源自肾上腺外副神经节瘤的儿茶酚胺危象的结果。T2WI 图像中的肾上腺磁共振成像 (MRI) 显示右肾门部有明显高强度和不均匀的肿块,大小为 50 × 56 × 79mm。右肾上腺切除术前尿儿茶酚胺的数据列于表 1。肾上腺素和去甲肾上腺素分泌过多,但多巴胺不分泌,通过 24 小时尿检证实。还观察到葡萄糖耐量受损。患者接受了 I-间碘苄胍 (I-MIBG) T2WI 图像中的肾上腺磁共振成像 (MRI) 显示右肾门部有明显高强度和不均匀的肿块,大小为 50 × 56 × 79mm。右肾上腺切除术前尿儿茶酚胺的数据列于表 1。肾上腺素和去甲肾上腺素分泌过多,但多巴胺不分泌,通过 24 小时尿检证实。还观察到葡萄糖耐量受损。患者接受了 I-间碘苄胍 (I-MIBG) T2WI 图像中的肾上腺磁共振成像 (MRI) 显示右肾门部有明显高强度和不均匀的肿块,大小为 50 × 56 × 79mm。右肾上腺切除术前尿儿茶酚胺的数据列于表 1。肾上腺素和去甲肾上腺素分泌过多,但多巴胺不分泌,通过 24 小时尿检证实。还观察到葡萄糖耐量受损。患者接受了 I-间碘苄胍 (I-MIBG) 还观察到葡萄糖耐量受损。患者接受了 I-间碘苄胍 (I-MIBG) 还观察到葡萄糖耐量受损。患者接受了 I-间碘苄胍 (I-MIBG)
更新日期:2020-01-22
中文翻译:
注射胰高血糖素后诊断为休克状态的肾上腺素为主的副神经节瘤一例
嗜铬细胞瘤-副神经节瘤 (PPGL) 是一种分泌儿茶酚胺的肿瘤,是一种罕见且可治愈的高血压病因,常伴有头痛、出汗、心悸和多汗症等并发症。PPGL 可能会与几种药物一起引发高血压危象,例如造影剂、胰高血糖素和甲氧氯普胺。我们报告了一例复发性右腹膜后副神经节瘤,在右肾上腺嗜铬细胞瘤手术后 17 年被诊断为高血压危象并给予胰高血糖素进行内镜检查预处理。一名 75 岁女性,患有头痛、阵发性高血压和多汗症 3 年,经内分泌和计算机断层扫描 (CT) 扫描诊断为嗜铬细胞瘤,1999 年显示右侧肾上腺肿瘤。大约 10 年后手术,她又患了阵发性高血压。2016年,她被安排进行胃镜检查。在胃镜检查前立即给予 1 mg 胰高血糖素以抑制胃肠蠕动。几分钟后,她震惊了。胃镜检查取消,转入我院急诊科。在最初的检查中,入院时的成像包括腹部 CT 扫描。增强 CT 扫描显示右肾门部有一个大小为 62 × 50mm 的明确肿块(图 1)。由于明显的高血压和心动过速,她接受了多学科治疗。静脉注射α-肾上腺素能阻滞剂酚妥拉明后,血压和脉搏逐渐得到控制。无嗜铬细胞瘤、副神经节瘤、在她的家族史中发现了或相关的遗传疾病(如 von Hippel-Lindau (VHL) 病)。考虑到之前已经进行了右侧全肾上腺切除术,这些生理学发现被认为是源自肾上腺外副神经节瘤的儿茶酚胺危象的结果。T2WI 图像中的肾上腺磁共振成像 (MRI) 显示右肾门部有明显高强度和不均匀的肿块,大小为 50 × 56 × 79mm。右肾上腺切除术前尿儿茶酚胺的数据列于表 1。肾上腺素和去甲肾上腺素的分泌过多,但不是多巴胺,通过 24 小时尿检证实。还观察到葡萄糖耐量受损。患者接受了 I-间碘苄胍 (I-MIBG) 考虑到之前已经进行了右侧全肾上腺切除术,这些生理学发现被认为是源自肾上腺外副神经节瘤的儿茶酚胺危象的结果。T2WI 图像中的肾上腺磁共振成像 (MRI) 显示右肾门部有明显高强度和不均匀的肿块,大小为 50 × 56 × 79mm。右肾上腺切除术前尿儿茶酚胺的数据列于表 1。肾上腺素和去甲肾上腺素分泌过多,但多巴胺不分泌,通过 24 小时尿检证实。还观察到葡萄糖耐量受损。患者接受了 I-间碘苄胍 (I-MIBG) 考虑到之前已经进行了右侧全肾上腺切除术,这些生理学发现被认为是源自肾上腺外副神经节瘤的儿茶酚胺危象的结果。T2WI 图像中的肾上腺磁共振成像 (MRI) 显示右肾门部有明显高强度和不均匀的肿块,大小为 50 × 56 × 79mm。右肾上腺切除术前尿儿茶酚胺的数据列于表 1。肾上腺素和去甲肾上腺素分泌过多,但多巴胺不分泌,通过 24 小时尿检证实。还观察到葡萄糖耐量受损。患者接受了 I-间碘苄胍 (I-MIBG) T2WI 图像中的肾上腺磁共振成像 (MRI) 显示右肾门部有明显高强度和不均匀的肿块,大小为 50 × 56 × 79mm。右肾上腺切除术前尿儿茶酚胺的数据列于表 1。肾上腺素和去甲肾上腺素分泌过多,但多巴胺不分泌,通过 24 小时尿检证实。还观察到葡萄糖耐量受损。患者接受了 I-间碘苄胍 (I-MIBG) T2WI 图像中的肾上腺磁共振成像 (MRI) 显示右肾门部有明显高强度和不均匀的肿块,大小为 50 × 56 × 79mm。右肾上腺切除术前尿儿茶酚胺的数据列于表 1。肾上腺素和去甲肾上腺素分泌过多,但多巴胺不分泌,通过 24 小时尿检证实。还观察到葡萄糖耐量受损。患者接受了 I-间碘苄胍 (I-MIBG) 还观察到葡萄糖耐量受损。患者接受了 I-间碘苄胍 (I-MIBG) 还观察到葡萄糖耐量受损。患者接受了 I-间碘苄胍 (I-MIBG)










































 京公网安备 11010802027423号
京公网安备 11010802027423号