当前位置:
X-MOL 学术
›
JAMA Dermatol.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
A Multicenter Cross-Sectional Study and Systematic Review of Necrobiotic Xanthogranuloma With Proposed Diagnostic Criteria.
JAMA Dermatology ( IF 11.5 ) Pub Date : 2020-01-15 , DOI: 10.1001/jamadermatol.2019.4221 Caroline A Nelson 1 , Connie S Zhong 2 , David A Hashemi 3 , Hovik J Ashchyan 4 , Zoe Brown-Joel 5 , Megan H Noe 6 , Sotonye Imadojemu 1 , Robert G Micheletti 6, 7 , Ruth Ann Vleugels 1 , Karolyn A Wanat 8 , Misha Rosenbach 6, 7 , Arash Mostaghimi 1
JAMA Dermatology ( IF 11.5 ) Pub Date : 2020-01-15 , DOI: 10.1001/jamadermatol.2019.4221 Caroline A Nelson 1 , Connie S Zhong 2 , David A Hashemi 3 , Hovik J Ashchyan 4 , Zoe Brown-Joel 5 , Megan H Noe 6 , Sotonye Imadojemu 1 , Robert G Micheletti 6, 7 , Ruth Ann Vleugels 1 , Karolyn A Wanat 8 , Misha Rosenbach 6, 7 , Arash Mostaghimi 1
Affiliation
|
Importance
Necrobiotic xanthogranuloma (NXG) is a non-Langerhans cell histiocytosis classically associated with paraproteinemia attributable to plasma-cell dyscrasias or lymphoproliferative disorders. Despite the morbidity of NXG, the literature is limited to case reports and small studies, and diagnostic criteria are lacking.
Objective
To evaluate the characteristics of NXG and propose diagnostic criteria.
Design, Setting, and Participants
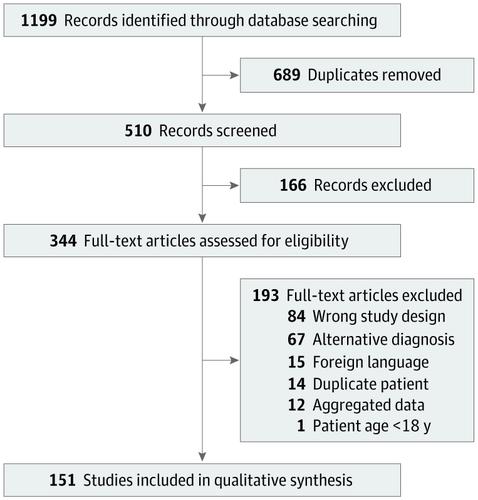
This multicenter cross-sectional study was conducted at tertiary academic referral centers and followed by a systematic review and a consensus exercise. The multicenter cohort included patients with NXG diagnosed at the Brigham and Women's and Massachusetts General Hospitals (2000-2018), the University of Iowa Hospitals and Clinics (2000-2018), and the University of Pennsylvania Health System (2008-2018). The systematic review was conducted in 2018 and included patients with NXG identified in the Cochrane, Ovid EMBASE, PubMed, and Web of Science databases. The consensus exercise was conducted by 8 board-certified dermatologists to identify diagnostic criteria.
Main Outcomes and Measures
Demographic factors, comorbidities, clinical features, and treatment response.
Results
Of 235 included patients with NXG (34 from the multicenter cohort and 201 from the systematic review results), the mean (SD) age at presentation was 61.6 (14.2) years; 147 (62.6%) were female. Paraproteinemia was detected in 193 patients (82.1%), most often IgG-κ (117 patients [50.0%]). A malignant condition was detected in 59 patients (25.1%), most often multiple myeloma (33 patients [14.0%]). The overall rate of paraproteinemia and/or a malignant condition was 83.8% (197 patients). In the multicenter cohort, evolution of paraproteinemia into multiple myeloma was observed up to 5.7 years (median [range], 2.4 [0.1-5.7] years) after NXG presentation. Cutaneous lesions consisted of papules, plaques, and/or nodules, typically yellow or orange in color (113 of 187 [60.4%]) with a periorbital distribution (130 of 219 [59.3%]). The eye was the leading site of extracutaneous involvement (34 of 235 [14.5%]). In the multicenter cohort, intravenous immunoglobulin had the best treatment response rate (9 of 9 patients [100%]), followed by antimalarial drugs (4 of 5 patients [80%]), intralesional triamcinolone (6 of 8 patients [75%]), surgery (3 of 4 patients [75%]), chemotherapy (8 of 12 patients [67%]), and lenalidomide or thalidomide (5 of 8 patients [63%]). The consensus exercise yielded 2 major criteria, which were (1) clinical and (2) histopathological features consistent with NXG, and 2 minor criteria, consisting of (1) paraproteinemia, plasma-cell dyscrasia, and/or other associated lymphoproliferative disorder and (2) periorbital distribution of cutaneous lesions. In the absence of foreign body, infection, or another identifiable cause, fulfillment of both major and at least 1 minor criterion were proposed to establish the diagnosis of NXG.
Conclusions and Relevance
Necrobiotic xanthogranuloma is a multisystem disorder associated with paraproteinemia and malignant conditions. The proposed diagnostic criteria may advance clinical research and should be validated.
中文翻译:

坏死性黄色肉芽肿的多中心横断面研究和系统评价以及拟议的诊断标准。
重要性 坏死性黄色肉芽肿 (NXG) 是一种非朗格汉斯细胞组织细胞增多症,通常与浆细胞恶液质或淋巴细胞增殖性疾病导致的副蛋白血症相关。尽管 NXG 发病率较高,但文献仅限于病例报告和小型研究,且缺乏诊断标准。目的评价NXG的特点并提出诊断标准。设计、设置和参与者 这项多中心横断面研究是在三级学术转诊中心进行的,随后进行了系统回顾和共识练习。多中心队列包括在布莱根妇女医院和马萨诸塞州总医院(2000-2018)、爱荷华大学医院和诊所(2000-2018)以及宾夕法尼亚大学卫生系统(2008-2018)诊断的 NXG 患者。该系统评价于 2018 年进行,纳入了 Cochrane、Ovid EMBASE、PubMed 和 Web of Science 数据库中发现的 NXG 患者。该共识由 8 名经过委员会认证的皮肤科医生进行,以确定诊断标准。主要结果和措施人口因素、合并症、临床特征和治疗反应。结果 在 235 名 NXG 患者中(34 名来自多中心队列,201 名来自系统评价结果),就诊时的平均 (SD) 年龄为 61.6 (14.2) 岁;147 名(62.6%)为女性。193 名患者 (82.1%) 检测到副蛋白血症,最常见的是 IgG-κ(117 名患者 [50.0%])。59 名患者 (25.1%) 被检测出恶性疾病,最常见的是多发性骨髓瘤 (33 名患者 [14.0%])。副蛋白血症和/或恶性疾病的总体发生率为 83.8%(197 名患者)。在多中心队列中,观察到 NXG 出现后长达 5.7 年(中位[范围],2.4 [0.1-5.7]年)副蛋白血症演变为多发性骨髓瘤。皮肤病变由丘疹、斑块和/或结节组成,通常呈黄色或橙色(187 例中的 113 例 [60.4%]),分布于眶周(219 例中的 130 例 [59.3%])。眼睛是皮外受累的主要部位(235 例中有 34 例 [14.5%])。在多中心队列中,静脉注射免疫球蛋白的治疗反应率最高(9 名患者中的 9 名 [100%]),其次是抗疟药物(5 名患者中的 4 名 [80%])、病灶内曲安奈德(8 名患者中的 6 名 [75%]) )、手术(4 名患者中的 3 名 [75%])、化疗(12 名患者中的 8 名 [67%])以及来那度胺或沙利度胺(8 名患者中的 5 名 [63%])。共识工作产生了 2 个主要标准,即 (1) 临床和 (2) 与 NXG 一致的组织病理学特征,以及 2 个次要标准,包括 (1) 副蛋白血症、浆细胞恶液质和/或其他相关的淋巴增殖性疾病和 ( 2)皮损分布于眶周。在没有异物、感染或其他可识别原因的情况下,建议满足主要标准和至少 1 个次要标准来确定 NXG 的诊断。结论和相关性 坏死性黄色肉芽肿是一种与副蛋白血症和恶性疾病相关的多系统疾病。拟议的诊断标准可能会推进临床研究,并且应该得到验证。
更新日期:2020-03-12
中文翻译:
坏死性黄色肉芽肿的多中心横断面研究和系统评价以及拟议的诊断标准。
重要性 坏死性黄色肉芽肿 (NXG) 是一种非朗格汉斯细胞组织细胞增多症,通常与浆细胞恶液质或淋巴细胞增殖性疾病导致的副蛋白血症相关。尽管 NXG 发病率较高,但文献仅限于病例报告和小型研究,且缺乏诊断标准。目的评价NXG的特点并提出诊断标准。设计、设置和参与者 这项多中心横断面研究是在三级学术转诊中心进行的,随后进行了系统回顾和共识练习。多中心队列包括在布莱根妇女医院和马萨诸塞州总医院(2000-2018)、爱荷华大学医院和诊所(2000-2018)以及宾夕法尼亚大学卫生系统(2008-2018)诊断的 NXG 患者。该系统评价于 2018 年进行,纳入了 Cochrane、Ovid EMBASE、PubMed 和 Web of Science 数据库中发现的 NXG 患者。该共识由 8 名经过委员会认证的皮肤科医生进行,以确定诊断标准。主要结果和措施人口因素、合并症、临床特征和治疗反应。结果 在 235 名 NXG 患者中(34 名来自多中心队列,201 名来自系统评价结果),就诊时的平均 (SD) 年龄为 61.6 (14.2) 岁;147 名(62.6%)为女性。193 名患者 (82.1%) 检测到副蛋白血症,最常见的是 IgG-κ(117 名患者 [50.0%])。59 名患者 (25.1%) 被检测出恶性疾病,最常见的是多发性骨髓瘤 (33 名患者 [14.0%])。副蛋白血症和/或恶性疾病的总体发生率为 83.8%(197 名患者)。在多中心队列中,观察到 NXG 出现后长达 5.7 年(中位[范围],2.4 [0.1-5.7]年)副蛋白血症演变为多发性骨髓瘤。皮肤病变由丘疹、斑块和/或结节组成,通常呈黄色或橙色(187 例中的 113 例 [60.4%]),分布于眶周(219 例中的 130 例 [59.3%])。眼睛是皮外受累的主要部位(235 例中有 34 例 [14.5%])。在多中心队列中,静脉注射免疫球蛋白的治疗反应率最高(9 名患者中的 9 名 [100%]),其次是抗疟药物(5 名患者中的 4 名 [80%])、病灶内曲安奈德(8 名患者中的 6 名 [75%]) )、手术(4 名患者中的 3 名 [75%])、化疗(12 名患者中的 8 名 [67%])以及来那度胺或沙利度胺(8 名患者中的 5 名 [63%])。共识工作产生了 2 个主要标准,即 (1) 临床和 (2) 与 NXG 一致的组织病理学特征,以及 2 个次要标准,包括 (1) 副蛋白血症、浆细胞恶液质和/或其他相关的淋巴增殖性疾病和 ( 2)皮损分布于眶周。在没有异物、感染或其他可识别原因的情况下,建议满足主要标准和至少 1 个次要标准来确定 NXG 的诊断。结论和相关性 坏死性黄色肉芽肿是一种与副蛋白血症和恶性疾病相关的多系统疾病。拟议的诊断标准可能会推进临床研究,并且应该得到验证。










































 京公网安备 11010802027423号
京公网安备 11010802027423号