当前位置:
X-MOL 学术
›
JAMA Intern. Med.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Effectiveness of Combined Behavioral and Drug Therapy for Overactive Bladder Symptoms in Men
JAMA Internal Medicine ( IF 22.5 ) Pub Date : 2020-03-01 , DOI: 10.1001/jamainternmed.2019.6398 Kathryn L Burgio 1, 2 , Stephen R Kraus 3 , Theodore M Johnson 4, 5 , Alayne D Markland 1, 2 , Camille P Vaughan 4, 5 , Peng Li 6, 7 , David T Redden 6 , Patricia S Goode 1, 2
JAMA Internal Medicine ( IF 22.5 ) Pub Date : 2020-03-01 , DOI: 10.1001/jamainternmed.2019.6398 Kathryn L Burgio 1, 2 , Stephen R Kraus 3 , Theodore M Johnson 4, 5 , Alayne D Markland 1, 2 , Camille P Vaughan 4, 5 , Peng Li 6, 7 , David T Redden 6 , Patricia S Goode 1, 2
Affiliation
|
Importance
First-line behavioral and drug therapies for overactive bladder (OAB) symptoms in men are effective but not usually curative. Objective
To determine whether combining behavioral and drug therapies improves outcomes compared with each therapy alone for OAB in men and to compare 3 sequences for implementing combined therapy. Design, Setting, and Participants
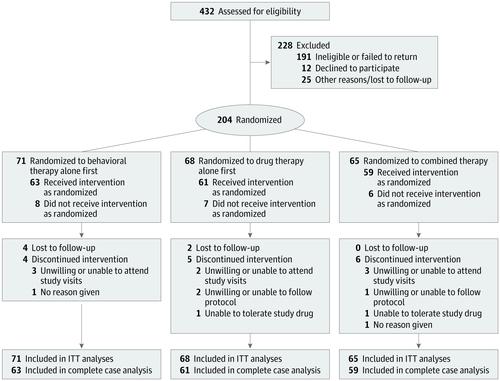
In this 3-site, 2-stage, 3-arm randomized clinical trial, participants were randomized to 6 weeks of behavioral therapy alone, drug therapy alone, or combined therapy followed by step-up to 6 weeks of combined therapy for all groups. Participants were recruited from 3 outpatient clinics and included community-dwelling men 40 years or older with urinary urgency and 9 or more voids per 24 hours. Data were collected from July 2010 to July 2015 and analyzed from April 2016 to September 2019. Interventions
Behavioral therapy consisted of pelvic floor muscle training with urge suppression strategies and delayed voiding. Drug therapy included an antimuscarinic (sustained-release tolterodine, 4 mg) plus an α-blocker (tamsulosin, 0.4 mg). Main Outcomes and Measures
Seven-day bladder diaries completed before and after each 6-week treatment stage were used to calculate reduction in frequency of urination (primary outcome) and other symptoms (ie, urgency, urgency incontinence, and nocturia). Other secondary outcomes included validated patient global ratings of improvement and satisfaction, Overactive Bladder Questionnaire score, and International Prostate Symptom Score. Results
Of the 204 included men, 133 (65.2%) were white, and the mean (SD) age was 64.1 (11.1) years. A total of 21 men discontinued treatment and 183 completed treatment. Mean (SD) voids per 24 hours decreased significantly in all 3 groups from baseline to 6-week follow-up (behavioral therapy: 11.7 [2.4] vs 8.8 [2.1]; change, 2.9 [2.4]; percentage change, 24.7%; P < .001; drug therapy: 11.8 [2.5] vs 10.3 [2.7]; change, 1.5 [2.3]; percentage change, 12.7%; P < .001; combined therapy: 11.8 [2.4] vs 8.2 [2.3]; change, 3.6 [2.1]; percentage change, 30.5%; P < .001). Intent-to-treat analyses indicated that posttreatment mean (SD) voiding frequencies were significantly lower in those receiving combined therapy compared with drug therapy alone (8.2 [2.3] vs 10.3 [2.7]; P < .001) but not significantly lower compared with those receiving behavioral therapy alone (8.2 [2.3] vs 8.8 [2.1]; P = .19) and were lower for behavioral therapy alone compared with drug therapy alone (8.8 [2.1] vs 10.3 [2.7]; P < .001). At 12-week follow-up, after all groups had received combined therapy, improvements in mean (SD) voids per 24 hours were also greatest for those receiving initial combined therapy compared with baseline (behavioral therapy: 11.7 [2.4] vs 8.0 [2.2]; change, 3.7 [2.3]; percentage change, 31.6%; P < .001; drug therapy: 11.8 [2.5] vs 8.6 [2.3]; change, 3.2 [2.5]; percentage change, 27.1%; P < .001; combined therapy: 11.8 [2.4] vs 8.0 [2.2]; change, 3.8 [2.1]; percentage change, 32.2%; P < .001), but there were no statistically significant group differences on primary or secondary measures. Conclusions and Relevance
Combining behavioral and drug therapy yields greater improvements in OAB symptoms than drug therapy alone but not behavioral therapy alone. When using a stepped approach, it is reasonable to begin with behavioral therapy alone. Trial Registration
ClinicalTrials.gov identifier: NCT01175382.
中文翻译:

行为和药物联合治疗对男性膀胱过度活动症状的有效性
重要性 针对男性膀胱过度活动症 (OAB) 症状的一线行为疗法和药物疗法是有效的,但通常不能治愈。目的 确定行为疗法和药物疗法相结合是否能改善男性 OAB 的单独治疗结果,并比较实施联合疗法的 3 个序列。设计、设置和参与者 在这项 3 地点、2 阶段、3 组随机临床试验中,参与者被随机分配到 6 周的单独行为治疗、单独药物治疗或联合治疗,然后逐步增加到 6 周所有组的联合治疗。参与者是从 3 个门诊招募的,包括 40 岁或以上的社区男性,患有尿急且每 24 小时排尿 9 次或更多。数据收集时间为 2010 年 7 月至 2015 年 7 月,分析时间为 2016 年 4 月至 2019 年 9 月。 干预 行为疗法包括盆底肌肉训练、冲动抑制策略和延迟排尿。药物治疗包括抗毒蕈碱(缓释托特罗定,4 毫克)加 α 受体阻滞剂(坦索罗辛,0.4 毫克)。主要结果和测量 在每个 6 周治疗阶段之前和之后完成的 7 天膀胱日记用于计算排尿频率(主要结果)和其他症状(即尿急、急迫性尿失禁和夜尿)的减少。其他次要结果包括经过验证的患者总体改善和满意度评分、膀胱过度活动问卷评分和国际前列腺症状评分。结果 在纳入的 204 名男性中,133 名 (65.2%) 是白人,平均 (SD) 年龄为 64.1 (11.1) 岁。共有 21 名男性停止治疗,183 人完成治疗。从基线到 6 周随访,所有 3 组每 24 小时的平均 (SD) 排尿量显着减少(行为治疗:11.7 [2.4] vs 8.8 [2.1];变化,2.9 [2.4];百分比变化,24.7%; P < .001;药物治疗:11.8 [2.5] vs 10.3 [2.7];变化,1.5 [2.3];百分比变化,12.7%;P < .001;联合治疗:11.8 [2.4] vs 8.2 [2.3];变化, 3.6 [2.1];百分比变化,30.5%;P < .001)。意向治疗分析表明,与单独药物治疗相比,接受联合治疗的患者的治疗后平均 (SD) 排尿频率显着较低(8.2 [2.3] vs 10.3 [2.7];P < .001),但与仅接受行为治疗的患者(8.2 [2.3] 对 8.8 [2.1];P = . 19) 并且与单独的药物治疗相比,单独的行为治疗较低(8.8 [2.1] vs 10.3 [2.7];P < .001)。在 12 周的随访中,所有组接受联合治疗后,与基线相比,接受初始联合治疗的组每 24 小时平均 (SD) 排尿的改善也最大(行为治疗:11.7 [2.4] vs 8.0 [2.2] ];变化,3.7 [2.3];变化百分比,31.6%;P < .001;药物治疗:11.8 [2.5] vs 8.6 [2.3];变化,3.2 [2.5];变化百分比,27.1%;P < .001 ;联合治疗:11.8 [2.4] vs 8.0 [2.2];变化,3.8 [2.1];百分比变化,32.2%;P < .001),但在主要或次要措施上没有统计学显着的组间差异。结论和相关性 行为疗法和药物疗法相结合比单独的药物疗法(但不是单独的行为疗法)在 OAB 症状方面产生更大的改善。当使用阶梯式方法时,从单独的行为疗法开始是合理的。试验注册 ClinicalTrials.gov 标识符:NCT01175382。
更新日期:2020-03-01
中文翻译:
行为和药物联合治疗对男性膀胱过度活动症状的有效性
重要性 针对男性膀胱过度活动症 (OAB) 症状的一线行为疗法和药物疗法是有效的,但通常不能治愈。目的 确定行为疗法和药物疗法相结合是否能改善男性 OAB 的单独治疗结果,并比较实施联合疗法的 3 个序列。设计、设置和参与者 在这项 3 地点、2 阶段、3 组随机临床试验中,参与者被随机分配到 6 周的单独行为治疗、单独药物治疗或联合治疗,然后逐步增加到 6 周所有组的联合治疗。参与者是从 3 个门诊招募的,包括 40 岁或以上的社区男性,患有尿急且每 24 小时排尿 9 次或更多。数据收集时间为 2010 年 7 月至 2015 年 7 月,分析时间为 2016 年 4 月至 2019 年 9 月。 干预 行为疗法包括盆底肌肉训练、冲动抑制策略和延迟排尿。药物治疗包括抗毒蕈碱(缓释托特罗定,4 毫克)加 α 受体阻滞剂(坦索罗辛,0.4 毫克)。主要结果和测量 在每个 6 周治疗阶段之前和之后完成的 7 天膀胱日记用于计算排尿频率(主要结果)和其他症状(即尿急、急迫性尿失禁和夜尿)的减少。其他次要结果包括经过验证的患者总体改善和满意度评分、膀胱过度活动问卷评分和国际前列腺症状评分。结果 在纳入的 204 名男性中,133 名 (65.2%) 是白人,平均 (SD) 年龄为 64.1 (11.1) 岁。共有 21 名男性停止治疗,183 人完成治疗。从基线到 6 周随访,所有 3 组每 24 小时的平均 (SD) 排尿量显着减少(行为治疗:11.7 [2.4] vs 8.8 [2.1];变化,2.9 [2.4];百分比变化,24.7%; P < .001;药物治疗:11.8 [2.5] vs 10.3 [2.7];变化,1.5 [2.3];百分比变化,12.7%;P < .001;联合治疗:11.8 [2.4] vs 8.2 [2.3];变化, 3.6 [2.1];百分比变化,30.5%;P < .001)。意向治疗分析表明,与单独药物治疗相比,接受联合治疗的患者的治疗后平均 (SD) 排尿频率显着较低(8.2 [2.3] vs 10.3 [2.7];P < .001),但与仅接受行为治疗的患者(8.2 [2.3] 对 8.8 [2.1];P = . 19) 并且与单独的药物治疗相比,单独的行为治疗较低(8.8 [2.1] vs 10.3 [2.7];P < .001)。在 12 周的随访中,所有组接受联合治疗后,与基线相比,接受初始联合治疗的组每 24 小时平均 (SD) 排尿的改善也最大(行为治疗:11.7 [2.4] vs 8.0 [2.2] ];变化,3.7 [2.3];变化百分比,31.6%;P < .001;药物治疗:11.8 [2.5] vs 8.6 [2.3];变化,3.2 [2.5];变化百分比,27.1%;P < .001 ;联合治疗:11.8 [2.4] vs 8.0 [2.2];变化,3.8 [2.1];百分比变化,32.2%;P < .001),但在主要或次要措施上没有统计学显着的组间差异。结论和相关性 行为疗法和药物疗法相结合比单独的药物疗法(但不是单独的行为疗法)在 OAB 症状方面产生更大的改善。当使用阶梯式方法时,从单独的行为疗法开始是合理的。试验注册 ClinicalTrials.gov 标识符:NCT01175382。










































 京公网安备 11010802027423号
京公网安备 11010802027423号