当前位置:
X-MOL 学术
›
Br. J. Surg.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Risk-adjusted benchmarks in laparoscopic liver surgery in a national cohort.
British Journal of Surgery ( IF 8.6 ) Pub Date : 2020-01-10 , DOI: 10.1002/bjs.11404 N Russolillo 1 , L Aldrighetti 2 , U Cillo 3 , A Guglielmi 4 , G M Ettorre 5 , F Giuliante 6 , V Mazzaferro 7 , R Dalla Valle 8 , L De Carlis 9 , E Jovine 10 , A Ferrero 1 ,
British Journal of Surgery ( IF 8.6 ) Pub Date : 2020-01-10 , DOI: 10.1002/bjs.11404 N Russolillo 1 , L Aldrighetti 2 , U Cillo 3 , A Guglielmi 4 , G M Ettorre 5 , F Giuliante 6 , V Mazzaferro 7 , R Dalla Valle 8 , L De Carlis 9 , E Jovine 10 , A Ferrero 1 ,
Affiliation
|
BACKGROUND
This study aimed to assess the best achievable outcomes in laparoscopic liver resection (LLR) after risk adjustment based on surgical technical difficulty using a national registry.
METHODS
LLRs registered in the Italian Group of Minimally Invasive Liver Surgery registry from November 2014 to March 2018 were considered. Benchmarks were calculated according to the Achievable Benchmark of Care (ABC™). LLRs at each centre were divided into three clusters (groups I, II and III) based on the Kawaguchi classification. ABCs for overall and major morbidity were calculated in each cluster. Multivariable analysis was used to identify independent risk factors for overall and major morbidity. Significant variables were used in further risk adjustment.
RESULTS
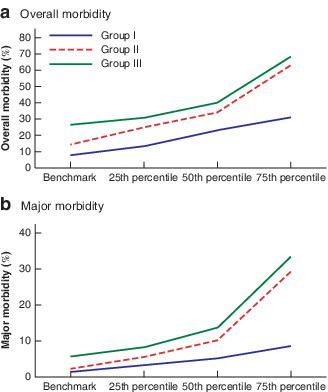
A total of 1752 of 2263 patients fulfilled the inclusion criteria: 1096 (62·6 per cent) in group I, 435 (24·8 per cent) in group II and 221 (12·6 per cent) in group III. The ABCs for overall morbidity (7·8, 14·2 and 26·4 per cent for grades I, II and II respectively) and major morbidity (1·4, 2·2 and 5·7 per cent) increased with the difficulty of LLR. Multivariable analysis showed an increased risk of overall morbidity associated with multiple LLRs (odds ratio (OR) 1·35), simultaneous intestinal resection (OR 3·76) and cirrhosis (OR 1·83), and an increased risk of major morbidity with intestinal resection (OR 4·61). ABCs for overall and major morbidity were 14·4 and 3·2 per cent respectively for multiple LLRs, 30 and 11·1 per cent for intestinal resection, and 14·9 and 4·8 per cent for cirrhosis.
CONCLUSION
Overall morbidity benchmarks for LLR ranged from 7·8 to 26·4 per cent, and those for major morbidity from 1·4 to 5·7 per cent, depending on complexity. Benchmark values should be adjusted according to multiple LLRs or simultaneous intestinal resection and cirrhosis.
ANTECEDENTES
Este estudio tuvo como objetivo evaluar los mejores resultados que se pueden conseguir en la resección hepática laparoscópica (laparoscopic liver resection, LLR) después del ajuste por riesgos basado en la dificultad de la técnica quirúrgica utilizando un registro nacional. MÉTODOS: Se consideraron las LLRs incluidas en el Registro del Grupo Italiano de Cirugía Hepática Mínimamente Invasiva desde 11/2014 a 03/2018. Los resultados de referencia (benchmarks) se calcularon de acuerdo con el Achievable Benchmark of Care (ABC™). Las LLRs de cada uno de los centros se dividieron en 3 grupos (Grupo I, II y III) en base a la clasificación de Kawaguchi. Se calculó el ABC de la morbilidad global y de la morbilidad mayor para cada grupo. Se realizó un análisis multivariable para identificar los factores independientes de riesgos para la morbilidad global y morbilidad mayor. Se utilizaron variables significativas para realizar ajustes de riesgo adicionales.
RESULTADOS
Un total de 1.752 pacientes de los 2.263 cumplían los criterios de inclusión, de los cuales 1.096 (62,6%) se incluyeron en el Grupo I, 435 (24,8%) en el Grupo II y 221 (12,6%) en el Grupo III. El ABC de la morbilidad global (7,8%, 14,2%, 26,4%) y de la morbilidad mayor (1,4%, 2,2%, 5,7%) aumentó del Grupo I al Grupo III. El análisis multivariable mostró un incremento del riesgo para la morbilidad global asociada con múltiples LLRs (razón de oportunidades, odds ratio, OR 1,349), resección intestinal simultánea (OR 3,760) y cirrosis (OR 1,825), y para la morbilidad mayor con la resección intestinal (OR 4,606). Los ABC de la morbilidad global y morbilidad mayor fueron 14,4% y 3,2% para las LLR múltiples, 30% y 11% para la resección intestinal, y 14,9% y 4,8% para la cirrosis, respectivamente. CONCLUSIÓN: Los resultados de referencia (benchmark) para la morbilidad global y morbilidad mayor en la LLR variaron entre un 8% y un 26% y entre un 1,4% y un 5,7%, dependiendo de la complejidad. Los valores de referencia deberían ajustarse de acuerdo con la práctica de LLRs múltiples o resección intestinal simultánea y cirrosis.
中文翻译:

全国人群腹腔镜肝手术中经过风险调整的基准。
背景技术本研究旨在评估使用国家注册中心基于手术技术难度调整风险后的腹腔镜肝切除术(LLR)最佳可达到的结果。方法考虑了2014年11月至2018年3月在意大利微创肝外科手术组意大利注册的LLR。根据可达到的护理基准(ABC™)计算基准。根据川口分类,将每个中心的LLR分为三个聚类(I,II和III组)。在每个组中计算总体和主要发病率的ABC。多变量分析用于确定总体和主要发病率的独立危险因素。在进一步的风险调整中使用了重要的变量。结果2263例患者中的1752例符合纳入标准:第一组为1096(62·6%),第二组为435(24·8%),第三组为221(12·6%)。总体发病率的ABC(I,II和II级分别为7%,8%,14·2和26·4%)和主要发病率(1-4%,2·2和5%·7%)随着困难的增加而增加LLR。多变量分析显示,与多个LLR(比值比(OR)1·35),同时进行肠切除术(OR 3·76)和肝硬化(OR 1·83)相关的总体发病风险增加,而患有大肠恶性肿瘤的主要发病风险增加。肠切除(OR 4·61)。多个LLR的总体发病率和主要发病率分别为14·4和3·2%,肠切除术的ABC为30·11·1%,肝硬化为14·9和4·8%。结论LLR的整体发病率基准介于7%,8%至26·4之间,根据复杂性的不同,主要发病率在1-4%到5%.7%之间。应根据多个LLR或同时进行肠切除和肝硬化来调整基准值。前瞻性评估洛斯马约克大学评估结果肝癌切除术(腹腔镜肝切除术,LLR)在普莱斯哥里斯戈斯州的巴西国立癌症研究中心得到了应用。墨多多斯:包括法人的注册商标在内的西班牙LLR包括11/2014 a 03/2018。达到可达到的护理基准(ABC™)的参考结果(基准)。Las LLRs de cada uno de los centros se dividieron en 3 grupos(Grupo I,II y III)在川口市的基地。环球全球市长和世界级市长帕拉卡达集团。全球多变的市长和全球多变的独立性分析家 实用变量显着地实现了对对象的调整。结果总计1.752人从洛斯2.263铜牌到洛斯瓜特斯,洛斯瓜伊斯1.096(62,6%)塞卢耶隆·恩·格鲁波一世,435(24,8%)埃尔·格鲁波二世221(12,6% )en el Grupo III。El ABC de la morbilidad global(7,8%,14,2%,26,4%)y de la morbilidad市长(1,4%,2,2%,5,7%) 。全球变数最小二乘法(razónde oportunidades,比值比,OR 1,349)结肠直肠切除术(OR 3,760)和cirrosis(OR 1,825),y re lacibilidad市长肠癌切除术(OR 4,606)。Los ABC de la morbilidad全球y morbilidad市长fueron 14.4%y 3,2%las LLR小肠,30%y 11%para laresección小肠,y 14,9%y 4,8%para la cirrosis,贝叶。结论:基准国家基准法院的审判结果(全球基准)和法拉利市长市长varariaron entun 8%y un 26%ent ent 1,4%y 5.7%,dependiendo de la complejidad。LLR的肠道异位症从肠道转移到肠道同时性和肝硬化。2%的准LLR杂种,30%的11%的肠段肠道,y的14.9%,4.8%的cirrosis,百叶草。结论:基准国家基准法院的审判结果(全球基准)和法拉利市长市长varariaron entun 8%y un 26%ent ent 1,4%y 5.7%,dependiendo de la complejidad。LLR的肠道异位症从肠道转移到肠道同时性和肝硬化。2%的准LLR杂种,30%的11%的肠段肠道,y的14.9%,4.8%的cirrosis,百叶草。结论:基准国家基准法院的审判结果(全球基准)和法拉利市长市长varariaron entun 8%y un 26%ent ent 1,4%y 5.7%,dependiendo de la complejidad。LLRs的肠道异位症,可同时缓解小肠粘膜炎和小肠粘膜炎。
更新日期:2020-01-10
中文翻译:
全国人群腹腔镜肝手术中经过风险调整的基准。
背景技术本研究旨在评估使用国家注册中心基于手术技术难度调整风险后的腹腔镜肝切除术(LLR)最佳可达到的结果。方法考虑了2014年11月至2018年3月在意大利微创肝外科手术组意大利注册的LLR。根据可达到的护理基准(ABC™)计算基准。根据川口分类,将每个中心的LLR分为三个聚类(I,II和III组)。在每个组中计算总体和主要发病率的ABC。多变量分析用于确定总体和主要发病率的独立危险因素。在进一步的风险调整中使用了重要的变量。结果2263例患者中的1752例符合纳入标准:第一组为1096(62·6%),第二组为435(24·8%),第三组为221(12·6%)。总体发病率的ABC(I,II和II级分别为7%,8%,14·2和26·4%)和主要发病率(1-4%,2·2和5%·7%)随着困难的增加而增加LLR。多变量分析显示,与多个LLR(比值比(OR)1·35),同时进行肠切除术(OR 3·76)和肝硬化(OR 1·83)相关的总体发病风险增加,而患有大肠恶性肿瘤的主要发病风险增加。肠切除(OR 4·61)。多个LLR的总体发病率和主要发病率分别为14·4和3·2%,肠切除术的ABC为30·11·1%,肝硬化为14·9和4·8%。结论LLR的整体发病率基准介于7%,8%至26·4之间,根据复杂性的不同,主要发病率在1-4%到5%.7%之间。应根据多个LLR或同时进行肠切除和肝硬化来调整基准值。前瞻性评估洛斯马约克大学评估结果肝癌切除术(腹腔镜肝切除术,LLR)在普莱斯哥里斯戈斯州的巴西国立癌症研究中心得到了应用。墨多多斯:包括法人的注册商标在内的西班牙LLR包括11/2014 a 03/2018。达到可达到的护理基准(ABC™)的参考结果(基准)。Las LLRs de cada uno de los centros se dividieron en 3 grupos(Grupo I,II y III)在川口市的基地。环球全球市长和世界级市长帕拉卡达集团。全球多变的市长和全球多变的独立性分析家 实用变量显着地实现了对对象的调整。结果总计1.752人从洛斯2.263铜牌到洛斯瓜特斯,洛斯瓜伊斯1.096(62,6%)塞卢耶隆·恩·格鲁波一世,435(24,8%)埃尔·格鲁波二世221(12,6% )en el Grupo III。El ABC de la morbilidad global(7,8%,14,2%,26,4%)y de la morbilidad市长(1,4%,2,2%,5,7%) 。全球变数最小二乘法(razónde oportunidades,比值比,OR 1,349)结肠直肠切除术(OR 3,760)和cirrosis(OR 1,825),y re lacibilidad市长肠癌切除术(OR 4,606)。Los ABC de la morbilidad全球y morbilidad市长fueron 14.4%y 3,2%las LLR小肠,30%y 11%para laresección小肠,y 14,9%y 4,8%para la cirrosis,贝叶。结论:基准国家基准法院的审判结果(全球基准)和法拉利市长市长varariaron entun 8%y un 26%ent ent 1,4%y 5.7%,dependiendo de la complejidad。LLR的肠道异位症从肠道转移到肠道同时性和肝硬化。2%的准LLR杂种,30%的11%的肠段肠道,y的14.9%,4.8%的cirrosis,百叶草。结论:基准国家基准法院的审判结果(全球基准)和法拉利市长市长varariaron entun 8%y un 26%ent ent 1,4%y 5.7%,dependiendo de la complejidad。LLR的肠道异位症从肠道转移到肠道同时性和肝硬化。2%的准LLR杂种,30%的11%的肠段肠道,y的14.9%,4.8%的cirrosis,百叶草。结论:基准国家基准法院的审判结果(全球基准)和法拉利市长市长varariaron entun 8%y un 26%ent ent 1,4%y 5.7%,dependiendo de la complejidad。LLRs的肠道异位症,可同时缓解小肠粘膜炎和小肠粘膜炎。










































 京公网安备 11010802027423号
京公网安备 11010802027423号