当前位置:
X-MOL 学术
›
JACC Cardiovasc. Inte.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Randomized Comparison Between Everolimus-Eluting Bioresorbable Scaffold and Metallic Stent: Multimodality Imaging Through 3 Years.
JACC: Cardiovascular Interventions ( IF 11.7 ) Pub Date : 2020-01-13 , DOI: 10.1016/j.jcin.2019.09.047 Yoshinobu Onuma 1 , Yasuhiro Honda 2 , Taku Asano 3 , Hiroki Shiomi 4 , Ken Kozuma 5 , Yukio Ozaki 6 , Atsuo Namiki 7 , Satoshi Yasuda 8 , Takafumi Ueno 9 , Kenji Ando 10 , Jungo Furuya 11 , Keiichi Igarashi Hanaoka 11 , Kengo Tanabe 12 , Kozo Okada 2 , Hideki Kitahara 2 , Masafumi Ono 3 , Hajime Kusano 13 , Richard Rapoza 13 , Charles Simonton 13 , Jeffrey J Popma 14 , Gregg W Stone 15 , Peter J Fitzgerald 2 , Patrick W Serruys 16 , Takeshi Kimura 4
JACC: Cardiovascular Interventions ( IF 11.7 ) Pub Date : 2020-01-13 , DOI: 10.1016/j.jcin.2019.09.047 Yoshinobu Onuma 1 , Yasuhiro Honda 2 , Taku Asano 3 , Hiroki Shiomi 4 , Ken Kozuma 5 , Yukio Ozaki 6 , Atsuo Namiki 7 , Satoshi Yasuda 8 , Takafumi Ueno 9 , Kenji Ando 10 , Jungo Furuya 11 , Keiichi Igarashi Hanaoka 11 , Kengo Tanabe 12 , Kozo Okada 2 , Hideki Kitahara 2 , Masafumi Ono 3 , Hajime Kusano 13 , Richard Rapoza 13 , Charles Simonton 13 , Jeffrey J Popma 14 , Gregg W Stone 15 , Peter J Fitzgerald 2 , Patrick W Serruys 16 , Takeshi Kimura 4
Affiliation
|
OBJECTIVES
The aim of this study was to investigate the vascular responses and fates of the scaffold after bioresorbable vascular scaffold (BVS) implantation using multimodality imaging.
BACKGROUND
Serial comprehensive image assessments after BVS implantation in the context of a randomized trial have not yet been reported.
METHODS
In the ABSORB Japan trial, 400 patients were randomized to a BVS (n = 266) or a cobalt-chromium everolimus-eluting stent (n = 134). Through 3 years, patients underwent serial angiography and intravascular ultrasound or optical coherence tomography (OCT).
RESULTS
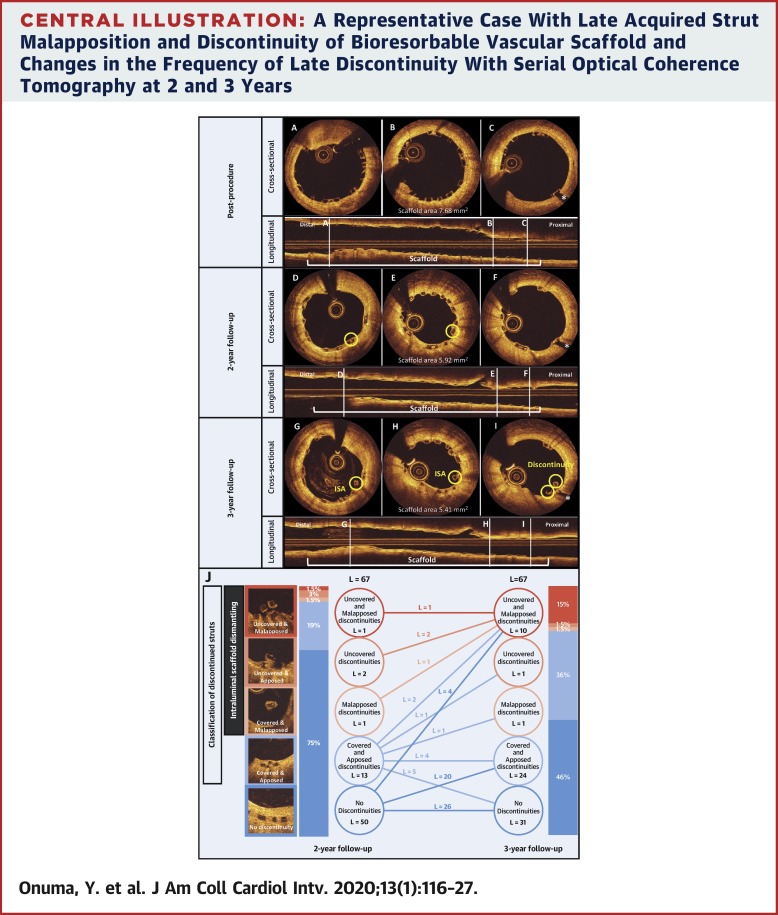
Luminal dimension at 3 years was consistently smaller with the BVS than with the cobalt-chromium everolimus-eluting stent (mean angiographic minimal luminal diameter 2.04 ± 0.63 mm vs. 2.40 ± 0.56 mm, mean difference -0.37 mm [95% confidence interval: -0.50 to -0.24 mm]; p < 0.001), mainly because of smaller device area (6.13 ± 2.03 mm2 vs. 7.15 ± 2.16 mm2, mean difference -1.04 mm2 [95% confidence interval: -1.66 to -0.42 mm2]; p < 0.001), and larger neointimal area (2.10 ± 0.61 mm2 vs. 1.86 ± 0.64 mm2, mean difference 0.24 mm2 [95% confidence interval: 0.06 to 0.43 mm2]; p = 0.01) by OCT. BVS-treated vessels did not show previously reported favorable vessel responses, such as positive vessel remodeling, late luminal enlargement, and restoration of vasomotion, although the OCT-based healing score was on average zero (interquartile range: 0.00 to 0.00). At 3 years, intraluminal scaffold dismantling (ISD) was observed in 14% of BVS. On serial OCT, ISD was observed in 6 lesions at 2 years, where the struts had been fully apposed at post-procedure, while ISD was observed in 12 lesions at 3 years, where 8 lesions were free from ISD on 2-year OCT. In 5 cases of very late scaffold thrombosis, strut discontinuities were detected in all 4 cases with available OCT immediately before reintervention.
CONCLUSIONS
In this multimodality serial imaging study, luminal dimension at 3 years was smaller with the BVS than with the cobalt-chromium everolimus-eluting stent. ISD, suspected to be one of the mechanisms of very late BVS thrombosis, was observed in a substantial proportion of cases at 3 years, which developed between post-procedure and 2 years and even beyond 2 years. (AVJ-301 Clinical Trial: A Clinical Evaluation of AVJ-301 [Absorb™ BVS] in Japanese Population [ABSORB JAPAN]; NCT01844284).
中文翻译:

依维莫司洗脱生物可吸收支架与金属支架之间的随机比较:3年多模态成像。
目的本研究的目的是通过多模式成像研究生物可吸收血管支架(BVS)植入后支架的血管反应和命运。背景技术尚未报道在随机试验的背景下进行BVS植入后的系列综合图像评估。方法在ABSORB Japan试验中,将400例患者随机分配到BVS(n = 266)或钴铬依维莫司洗脱支架(n = 134)中。经过3年,患者接受了连续血管造影和血管内超声检查或光学相干断层扫描(OCT)。结果BVS在3年时的管腔尺寸始终小于钴-铬依维莫司洗脱支架(平均血管造影最小管腔直径2.04±0.63 mm与2.40±0.56 mm,平均差-0.37 mm [95%置信区间: -0。50至-0.24毫米];p <0.001),主要是由于较小的器械面积(6.13±2.03 mm2 vs. 7.15±2.16 mm2,平均差异-1.04 mm2 [95%置信区间:-1.66至-0.42 mm2; p <0.001),以及新内膜较大面积(OCT)(2.10±0.61 mm2与1.86±0.64 mm2,平均差0.24 mm2 [95%置信区间:0.06至0.43 mm2]; p = 0.01)。尽管基于OCT的愈合评分平均为零(四分位间距:0.00至0.00),但BVS治疗的血管未显示出先前报道的良好血管反应,例如正的血管重塑,晚期管腔增大和血管舒张恢复。在3年时,在14%的BVS中观察到腔内支架拆除(ISD)。在连续OCT上,第2年在6个病变中观察到了ISD,手术后这些撑杆已完全并入,在3年时的12个病变中观察到ISD,在2年的OCT上有8个病变没有ISD。在5例非常晚期的支架血栓形成中,所有4例在重新干预前即刻可用OCT的病例中均检测到支杆不连续。结论在这项多模态系列成像研究中,BVS的3年腔尺寸比钴铬依维莫司洗脱支架小。ISD被怀疑是BVS晚期血栓形成的机制之一,在3年的相当大比例的病例中观察到了ISD,其发生在术后2年甚至超过2年之间。(AVJ-301临床试验:AVJ-301 [Absorb™BVS]在日本人群中的临床评估[ABSORB JAPAN]; NCT01844284)。在重新干预之前,在所有可用OCT的4例患者中均检测到支杆不连续。结论在这项多模态系列成像研究中,BVS的3年腔尺寸比钴铬依维莫司洗脱支架小。ISD被怀疑是BVS晚期血栓形成的机制之一,在3年的相当大比例的病例中观察到了ISD,其发生在术后2年甚至超过2年之间。(AVJ-301临床试验:AVJ-301 [Absorb™BVS]在日本人群中的临床评估[ABSORB JAPAN]; NCT01844284)。在重新干预之前,在所有可用OCT的4例患者中均检测到支杆不连续。结论在这项多模态系列成像研究中,BVS的3年腔尺寸比钴铬依维莫司洗脱支架小。ISD被怀疑是BVS晚期血栓形成的机制之一,在3年的相当大比例的病例中观察到了ISD,其发生在术后2年甚至超过2年之间。(AVJ-301临床试验:AVJ-301 [Absorb™BVS]在日本人群中的临床评估[ABSORB JAPAN]; NCT01844284)。BVS在3年时的管腔尺寸小于钴-铬依维莫司洗脱支架。ISD被怀疑是BVS晚期血栓形成的机制之一,在3年的相当大比例的病例中观察到了ISD,其发生在术后2年甚至超过2年之间。(AVJ-301临床试验:AVJ-301 [Absorb™BVS]在日本人群中的临床评估[ABSORB JAPAN]; NCT01844284)。BVS在3年时的管腔尺寸小于钴-铬依维莫司洗脱支架。ISD被怀疑是BVS晚期血栓形成的机制之一,在3年的相当大比例的病例中观察到了ISD,其发生在术后2年甚至超过2年之间。(AVJ-301临床试验:AVJ-301 [Absorb™BVS]在日本人群中的临床评估[ABSORB JAPAN]; NCT01844284)。
更新日期:2020-01-07
中文翻译:
依维莫司洗脱生物可吸收支架与金属支架之间的随机比较:3年多模态成像。
目的本研究的目的是通过多模式成像研究生物可吸收血管支架(BVS)植入后支架的血管反应和命运。背景技术尚未报道在随机试验的背景下进行BVS植入后的系列综合图像评估。方法在ABSORB Japan试验中,将400例患者随机分配到BVS(n = 266)或钴铬依维莫司洗脱支架(n = 134)中。经过3年,患者接受了连续血管造影和血管内超声检查或光学相干断层扫描(OCT)。结果BVS在3年时的管腔尺寸始终小于钴-铬依维莫司洗脱支架(平均血管造影最小管腔直径2.04±0.63 mm与2.40±0.56 mm,平均差-0.37 mm [95%置信区间: -0。50至-0.24毫米];p <0.001),主要是由于较小的器械面积(6.13±2.03 mm2 vs. 7.15±2.16 mm2,平均差异-1.04 mm2 [95%置信区间:-1.66至-0.42 mm2; p <0.001),以及新内膜较大面积(OCT)(2.10±0.61 mm2与1.86±0.64 mm2,平均差0.24 mm2 [95%置信区间:0.06至0.43 mm2]; p = 0.01)。尽管基于OCT的愈合评分平均为零(四分位间距:0.00至0.00),但BVS治疗的血管未显示出先前报道的良好血管反应,例如正的血管重塑,晚期管腔增大和血管舒张恢复。在3年时,在14%的BVS中观察到腔内支架拆除(ISD)。在连续OCT上,第2年在6个病变中观察到了ISD,手术后这些撑杆已完全并入,在3年时的12个病变中观察到ISD,在2年的OCT上有8个病变没有ISD。在5例非常晚期的支架血栓形成中,所有4例在重新干预前即刻可用OCT的病例中均检测到支杆不连续。结论在这项多模态系列成像研究中,BVS的3年腔尺寸比钴铬依维莫司洗脱支架小。ISD被怀疑是BVS晚期血栓形成的机制之一,在3年的相当大比例的病例中观察到了ISD,其发生在术后2年甚至超过2年之间。(AVJ-301临床试验:AVJ-301 [Absorb™BVS]在日本人群中的临床评估[ABSORB JAPAN]; NCT01844284)。在重新干预之前,在所有可用OCT的4例患者中均检测到支杆不连续。结论在这项多模态系列成像研究中,BVS的3年腔尺寸比钴铬依维莫司洗脱支架小。ISD被怀疑是BVS晚期血栓形成的机制之一,在3年的相当大比例的病例中观察到了ISD,其发生在术后2年甚至超过2年之间。(AVJ-301临床试验:AVJ-301 [Absorb™BVS]在日本人群中的临床评估[ABSORB JAPAN]; NCT01844284)。在重新干预之前,在所有可用OCT的4例患者中均检测到支杆不连续。结论在这项多模态系列成像研究中,BVS的3年腔尺寸比钴铬依维莫司洗脱支架小。ISD被怀疑是BVS晚期血栓形成的机制之一,在3年的相当大比例的病例中观察到了ISD,其发生在术后2年甚至超过2年之间。(AVJ-301临床试验:AVJ-301 [Absorb™BVS]在日本人群中的临床评估[ABSORB JAPAN]; NCT01844284)。BVS在3年时的管腔尺寸小于钴-铬依维莫司洗脱支架。ISD被怀疑是BVS晚期血栓形成的机制之一,在3年的相当大比例的病例中观察到了ISD,其发生在术后2年甚至超过2年之间。(AVJ-301临床试验:AVJ-301 [Absorb™BVS]在日本人群中的临床评估[ABSORB JAPAN]; NCT01844284)。BVS在3年时的管腔尺寸小于钴-铬依维莫司洗脱支架。ISD被怀疑是BVS晚期血栓形成的机制之一,在3年的相当大比例的病例中观察到了ISD,其发生在术后2年甚至超过2年之间。(AVJ-301临床试验:AVJ-301 [Absorb™BVS]在日本人群中的临床评估[ABSORB JAPAN]; NCT01844284)。










































 京公网安备 11010802027423号
京公网安备 11010802027423号