Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Association of Medicaid Expansion With 1-Year Mortality Among Patients With End-Stage Renal Disease
JAMA ( IF 63.1 ) Pub Date : 2018-12-04 , DOI: 10.1001/jama.2018.16504 Shailender Swaminathan 1, 2, 3, 4 , Benjamin D. Sommers 5, 6 , Rebecca Thorsness 1 , Rajnish Mehrotra 7 , Yoojin Lee 1 , Amal N. Trivedi 1, 2
JAMA ( IF 63.1 ) Pub Date : 2018-12-04 , DOI: 10.1001/jama.2018.16504 Shailender Swaminathan 1, 2, 3, 4 , Benjamin D. Sommers 5, 6 , Rebecca Thorsness 1 , Rajnish Mehrotra 7 , Yoojin Lee 1 , Amal N. Trivedi 1, 2
Affiliation
|
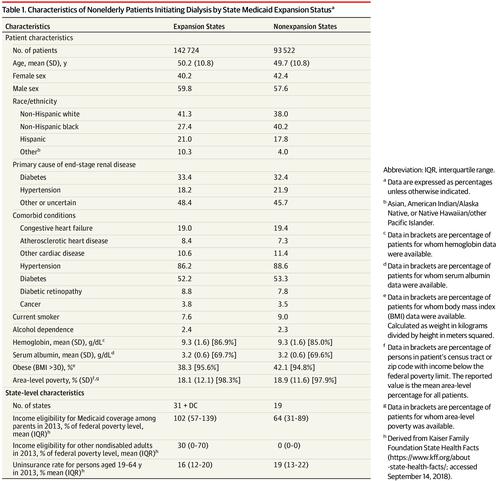
Importance The Affordable Care Act Medicaid expansion may be associated with reduced mortality, but evidence to date is limited. Patients with end-stage renal disease (ESRD) are a high-risk group that may be particularly affected by Medicaid expansion. Objective To examine the association of Medicaid expansion with 1-year mortality among nonelderly patients with ESRD initiating dialysis. Design, Setting, and Participants Difference-in-differences analysis of nonelderly patients initiating dialysis in Medicaid expansion and nonexpansion states from January 2011 to March 2017. Exposure Living in a Medicaid expansion state. Main Outcomes and Measures The primary outcome was 1-year mortality. Secondary outcomes were insurance, predialysis nephrology care, and type of vascular access for hemodialysis. Results A total of 142 724 patients in expansion states (mean age, 50.2 years; 40.2% women) and 93 522 patients in nonexpansion states (mean age, 49.7; 42.4% women) were included. In Medicaid expansion states, 1-year mortality following dialysis initiation declined from 6.9% in the preexpansion period to 6.1% after expansion (change, −0.8 percentage points; 95% CI, −1.1 to −0.5). In nonexpansion states, mortality rates were 7.0% before expansion and 6.8% after expansion (change, −0.2 percentage points; 95% CI, −0.5 to 0.2), yielding an adjusted absolute reduction in mortality in expansion states of −0.6 percentage points (95% CI, −1.0 to −0.2). Mortality reductions were largest for black patients (−1.4 percentage points; 95% CI, −2.2, −0.7; P=.04 for interaction) and patients aged 19 to 44 years (−1.1 percentage points; 95% CI, −2.1 to −0.3; P=.01 for interaction). Expansion was associated with a 10.5-percentage-point (95% CI, 7.7-13.2) increase in Medicaid coverage at dialysis initiation, a −4.2-percentage-point (95% CI, −6.0 to −2.3) decrease in being uninsured, and a 2.3-percentage-point (95% CI, 0.6-4.1) increase in the presence of an arteriovenous fistula or graft. Changes in predialysis nephrology care were not significant. Conclusions and Relevance Among patients with ESRD initiating dialysis, living in a state that expanded Medicaid under the Affordable Care Act was associated with lower 1-year mortality. If this association is causal, further research is needed to understand what factors may have contributed to this finding.
中文翻译:

医疗补助扩张与终末期肾病患者 1 年死亡率的关联
重要性 《平价医疗法案》扩大医疗补助可能与降低死亡率有关,但迄今为止的证据有限。终末期肾病 (ESRD) 患者是一个高危人群,可能特别受医疗补助计划的影响。目的 旨在检查医疗补助扩大与非老年 ESRD 患者开始透析的 1 年死亡率之间的关联。设计、设置和参与者 2011 年 1 月至 2017 年 3 月在医疗补助扩展和非扩展状态下开始透析的非老年患者的差异分析。暴露生活在医疗补助扩展状态。主要结果和措施 主要结果是 1 年死亡率。次要结果是保险、透析前肾脏病学护理和血液透析的血管通路类型。结果共纳入142 724例扩张状态患者(平均年龄50.2岁;40.2%女性)和93 522例非扩张状态患者(平均年龄49.7;42.4%女性)。在医疗补助扩张州,透析开始后的 1 年死亡率从扩张前的 6.9% 下降到扩张后的 6.1%(变化,-0.8 个百分点;95% CI,-1.1 至 -0.5)。在非扩张状态下,扩张前的死亡率为 7.0%,扩张后为 6.8%(变化,-0.2 个百分点;95% CI,-0.5 至 0.2),在扩张状态下调整后的死亡率绝对降低为 -0.6 个百分点( 95% CI,-1.0 至 -0.2)。黑人患者(-1.4 个百分点;95% CI,-2.2,-0.7;交互作用 P=.04)和 19 至 44 岁患者(-1.1 个百分点;95% CI,-2.1 至-0.3;P=。01 进行交互)。扩张与透析开始时医疗补助覆盖率增加 10.5 个百分点(95% CI,7.7-13.2)相关,未投保减少 -4.2 个百分点(95% CI,-6.0 至 -2.3),在存在动静脉瘘或移植物的情况下增加 2.3 个百分点(95% CI,0.6-4.1)。透析前肾脏病学护理的变化并不显着。结论和相关性 在开始透析的 ESRD 患者中,生活在根据平价医疗法案扩大医疗补助的州与较低的 1 年死亡率相关。如果这种关联是因果关系,则需要进一步研究以了解可能导致这一发现的因素。未投保者减少 2 个百分点(95% CI,-6.0 至 -2.3),存在动静脉瘘或移植物时增加 2.3 个百分点(95% CI,0.6-4.1)。透析前肾脏病学护理的变化并不显着。结论和相关性 在开始透析的 ESRD 患者中,生活在根据平价医疗法案扩大医疗补助的州与较低的 1 年死亡率相关。如果这种关联是因果关系,则需要进一步研究以了解可能导致这一发现的因素。未投保者减少 2 个百分点(95% CI,-6.0 至 -2.3),存在动静脉瘘或移植物时增加 2.3 个百分点(95% CI,0.6-4.1)。透析前肾脏病学护理的变化并不显着。结论和相关性 在开始透析的 ESRD 患者中,生活在根据平价医疗法案扩大医疗补助的州与较低的 1 年死亡率相关。如果这种关联是因果关系,则需要进一步研究以了解可能导致这一发现的因素。生活在根据“平价医疗法案”扩大医疗补助的州与较低的 1 年死亡率相关。如果这种关联是因果关系,则需要进一步研究以了解可能导致这一发现的因素。生活在根据“平价医疗法案”扩大医疗补助的州与较低的 1 年死亡率相关。如果这种关联是因果关系,则需要进一步研究以了解可能导致这一发现的因素。
更新日期:2018-12-04
中文翻译:
医疗补助扩张与终末期肾病患者 1 年死亡率的关联
重要性 《平价医疗法案》扩大医疗补助可能与降低死亡率有关,但迄今为止的证据有限。终末期肾病 (ESRD) 患者是一个高危人群,可能特别受医疗补助计划的影响。目的 旨在检查医疗补助扩大与非老年 ESRD 患者开始透析的 1 年死亡率之间的关联。设计、设置和参与者 2011 年 1 月至 2017 年 3 月在医疗补助扩展和非扩展状态下开始透析的非老年患者的差异分析。暴露生活在医疗补助扩展状态。主要结果和措施 主要结果是 1 年死亡率。次要结果是保险、透析前肾脏病学护理和血液透析的血管通路类型。结果共纳入142 724例扩张状态患者(平均年龄50.2岁;40.2%女性)和93 522例非扩张状态患者(平均年龄49.7;42.4%女性)。在医疗补助扩张州,透析开始后的 1 年死亡率从扩张前的 6.9% 下降到扩张后的 6.1%(变化,-0.8 个百分点;95% CI,-1.1 至 -0.5)。在非扩张状态下,扩张前的死亡率为 7.0%,扩张后为 6.8%(变化,-0.2 个百分点;95% CI,-0.5 至 0.2),在扩张状态下调整后的死亡率绝对降低为 -0.6 个百分点( 95% CI,-1.0 至 -0.2)。黑人患者(-1.4 个百分点;95% CI,-2.2,-0.7;交互作用 P=.04)和 19 至 44 岁患者(-1.1 个百分点;95% CI,-2.1 至-0.3;P=。01 进行交互)。扩张与透析开始时医疗补助覆盖率增加 10.5 个百分点(95% CI,7.7-13.2)相关,未投保减少 -4.2 个百分点(95% CI,-6.0 至 -2.3),在存在动静脉瘘或移植物的情况下增加 2.3 个百分点(95% CI,0.6-4.1)。透析前肾脏病学护理的变化并不显着。结论和相关性 在开始透析的 ESRD 患者中,生活在根据平价医疗法案扩大医疗补助的州与较低的 1 年死亡率相关。如果这种关联是因果关系,则需要进一步研究以了解可能导致这一发现的因素。未投保者减少 2 个百分点(95% CI,-6.0 至 -2.3),存在动静脉瘘或移植物时增加 2.3 个百分点(95% CI,0.6-4.1)。透析前肾脏病学护理的变化并不显着。结论和相关性 在开始透析的 ESRD 患者中,生活在根据平价医疗法案扩大医疗补助的州与较低的 1 年死亡率相关。如果这种关联是因果关系,则需要进一步研究以了解可能导致这一发现的因素。未投保者减少 2 个百分点(95% CI,-6.0 至 -2.3),存在动静脉瘘或移植物时增加 2.3 个百分点(95% CI,0.6-4.1)。透析前肾脏病学护理的变化并不显着。结论和相关性 在开始透析的 ESRD 患者中,生活在根据平价医疗法案扩大医疗补助的州与较低的 1 年死亡率相关。如果这种关联是因果关系,则需要进一步研究以了解可能导致这一发现的因素。生活在根据“平价医疗法案”扩大医疗补助的州与较低的 1 年死亡率相关。如果这种关联是因果关系,则需要进一步研究以了解可能导致这一发现的因素。生活在根据“平价医疗法案”扩大医疗补助的州与较低的 1 年死亡率相关。如果这种关联是因果关系,则需要进一步研究以了解可能导致这一发现的因素。










































 京公网安备 11010802027423号
京公网安备 11010802027423号