JAMA Surgery ( IF 15.7 ) Pub Date : 2018-10-01 , DOI: 10.1001/jamasurg.2018.2721 Zheng Li 1 , Zhengqing Lei 1 , Yong Xia 1 , Jun Li 1 , Kui Wang 1 , Han Zhang 1 , Xuying Wan 1 , Tian Yang 1 , Weiping Zhou 1 , Mengchao Wu 1 , Timothy M. Pawlik 2 , Wan Yee Lau 3 , Feng Shen 1
|
Importance A reduced incidence of microvascular invasion (MVI) in hepatitis B virus (HBV)–related hepatocellular carcinoma (HCC) may be associated with a decreased risk of early tumor recurrence and better survival after partial hepatectomy.
Objective To examine the association of preoperative antiviral treatment (AVT) with the incidences of MVI and posthepatectomy early tumor recurrence in HBV-related HCC.
Design, Setting, and Participants Data on a cohort of 2362 patients who underwent R0 resection for HBV-related HCC between January 2008 and April 2010 at the Eastern Hepatobiliary Surgery Hospital, Second Military Medical University, Shanghai, China, were reviewed. The median (interquartile range) postoperative follow-up was 44.8 (22.8-59.3) months. Data were analyzed from June 2016 to October 2017.
Interventions Preoperative AVT and partial hepatectomy.
Main Outcomes and Measures Overall survival and time to recurrence after surgery were calculated and compared using the Kaplan-Meier method, log-rank test, and Cox regression analysis. Independent risk factors of MVI presence were assessed by logistic regression analysis.
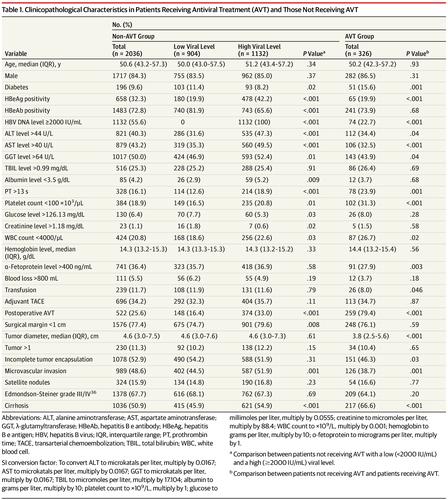
Results Among 2362 included patients, 1999 (84.6%) were men, and the median (interquartile range) age was 50.6 (43.1-57.3) years. A total of 2036 patients (86.2%) did not receive any preoperative AVT, while 326 (13.8%) received ongoing AVT more than 90 days before surgery. In the non-AVT group, compared with a preoperative HBV DNA level of less than 2000 IU/mL, a preoperative HBV DNA level of 2000 IU/mL or greater was associated with an increased risk of MVI (odds ratio [OR], 1.399; 95% CI, 1.151-1.701). Compared with the non-AVT group, patients receiving AVT had a lower incidence of MVI (38.7% [126 of 326] vs 48.6% [989 of 2036]; P = .001) and reduced risk of MVI (OR, 0.758; 95% CI, 0.575-0.998). A complete response to AVT was an independent protective factor of MVI (OR, 0.690; 95% CI, 0.500-0.952). Accordingly, preoperative AVT was associated with decreased 6-month, 1-year, and 2-year recurrences vs non-AVT (14.2%, 24.6%, and 38.5%, respectively, vs 23.4%, 37.1%, and 52.3%; P < .001); AVT was protective of early tumor recurrence (hazard ratio, 0.732; 95% CI, 0.605-0.886). In addition, patients in the non-AVT group were more likely to have multiple intrahepatic recurrences (49.1% [549 of 1119] vs 36.2% [54 of 149]; P = .003) and recurrences involving multiple hepatic segments compared with patients receiving AVT.
Conclusions and Relevance A high preoperative HBV DNA level was an independent risk factor of MVI. Antiviral treatment administered more than 90 days before surgery was associated with reduced incidences of MVI and early tumor recurrence after partial hepatectomy for HBV-related HCC.
中文翻译:
术前抗病毒治疗与乙型肝炎病毒相关的肝细胞癌的微血管浸润和肿瘤早期复发的发生率相关
重要性 乙型肝炎病毒(HBV)相关的肝细胞癌(HCC)中微血管侵袭(MVI)发生率的降低可能与早期肿瘤复发的风险降低以及部分肝切除术后更好的生存率相关。
目的 探讨HBV相关HCC的术前抗病毒治疗(AVT)与MVI的发生率和肝切除术后早期肿瘤复发的关系。
设计,背景和参与者的 数据收集了2008年1月至2010年4月在中国第二军医大学东方肝胆外科医院接受HBV相关性HCC R0切除术的2362名患者的研究数据。术后中位随访时间(四分位间距)为44.8(22.8-59.3)个月。分析了2016年6月至2017年10月的数据。
干预 术前AVT和部分肝切除术。
主要结果和措施 使用Kaplan-Meier方法,对数秩检验和Cox回归分析计算并比较了手术后的总生存期和复发时间。通过Logistic回归分析评估MVI存在的独立危险因素。
结果 在2362名患者中,1999年(84.6%)为男性,中位(四分位间距)年龄为50.6(43.1-57.3)岁。共有2036例患者(86.2%)未接受任何术前AVT,而326例(13.8%)在手术前90天以上接受了持续性AVT。在非AVT组中,与术前HBV DNA水平低于2000 IU / mL相比,术前HBV DNA水平为2000 IU / mL或更高与MVI风险增加相关(比值比[OR]为1.399 ; 95%CI,1.15-1.701)。与非AVT组相比,接受AVT的患者的MVI发生率较低(38.7%[326 of 126] vs 48.6%[2036 989];P = .001)和降低的MVI风险(OR,0.758; 95%CI,0.575-0.998)。对AVT的完全反应是MVI的独立保护因子(OR,0.690; 95%CI,0.500-0.952)。因此,与非AVT相比,术前AVT与6个月,1年和2年复发率降低相关(分别为14.2%,24.6%和38.5%,而23.4%,37.1%和52.3%;P <.001); AVT可预防早期肿瘤复发(危险比,0.732; 95%CI,0.605-0.886)。另外,与接受治疗的患者相比,非AVT组的患者更有可能发生多次肝内复发(49.1%[1119的549]对36.2%[54 149的P ];P = .003),并且涉及多个肝段的复发AVT。
结论和相关性 术前HBV DNA高水平是MVI的独立危险因素。术前90天以上进行抗病毒治疗与HBV相关性HCC部分肝切除术后MVI发生率降低和早期肿瘤复发相关。










































 京公网安备 11010802027423号
京公网安备 11010802027423号