JAMA Surgery ( IF 16.9 ) Pub Date : 2018-10-01 , DOI: 10.1001/jamasurg.2018.2089 Jae Pil Jung 1 , Mazen S. Zenati 1 , Mashaal Dhir 2 , Amer H. Zureikat 1 , Herbert J. Zeh 1 , Richard L. Simmons 3 , Melissa E. Hogg 1
|
Importance Technical proficiency at robotic pancreaticoduodenectomy (RPD) and video assessment are promising tools for understanding postoperative outcomes. Delayed gastric emptying (DGE) remains a major driver of cost and morbidity after pancreaticoduodenectomy.
Objective To determine if technical variables during RPD are associated with postoperative DGE.
Design, Setting, and Participants A retrospective study was conducted of technical assessment performed in all available videos (n = 192) of consecutive RPDs performed at a single academic institution from October 3, 2008, through September 27, 2016.
Exposures Video review of gastrojejunal anastomosis during RPD.
Main Outcomes and Measures Delayed gastric emptying was classified according to International Study Group of Pancreatic Surgery criteria. Video analysis reviewed technical variables specific in the construction of the gastrojejunal anastomosis. Using multivariate analysis, DGE was correlated with known patient variables and technical variables, individually and combined.
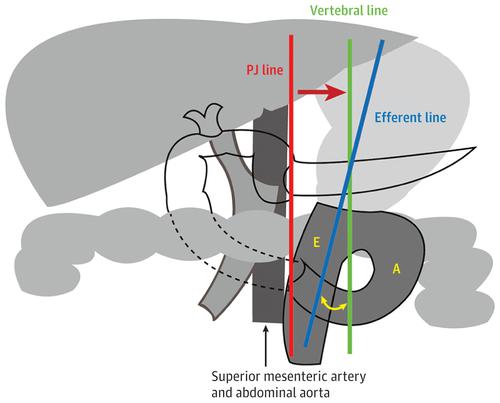
Results Of 410 RPDs performed, video was available for 192 RPDs (80 women and 112 men; mean [SD] age, 65.7 [11.1] years). Delayed gastric emptying occurred in 41 patients (21.4%; grade A, 15; grade B, 14; and grade C, 12). Patient variables contributing to DGE on multivariate analysis were advanced age (odds ratio [OR] 1.11; 95% CI, 1.05-1.16; P < .001), small pancreatic duct size (OR, 0.84; 95% CI, 0.72-0.98; P = .03), and postoperative pseudoaneurysm (OR, 17.29; 95% CI, 2.34-127.78; P = .005). However, technical variables contributing to decreased DGE on multivariate analysis included the flow angle (within 30° of vertical) between the stomach and efferent jejunal limb (OR, 0.25; 95% CI, 0.08-0.79; P = .02), greater length of the gastrojejunal anastomosis (OR, 0.40; 95% CI, 0.20-0.77; P = .006), and a robotic-sewn anastomosis (robotic suture vs stapler: OR, 0.30; 95% CI, 0.09-0.95; P = .04).
Conclusions and Relevance This study examines modifiable technical factors through the use of review of video obtained at the time of operation and suggests ways by which the surgical construction of the gastrojejunal anastomosis during RPD may reduce the incidence of DGE as a framework for prospective quality improvement.
中文翻译:
使用视频审查来调查胰十二指肠切除术后可能与胃排空延迟有关的技术因素
重要性 机器人胰十二指肠切除术(RPD)的技术水平和视频评估是了解术后结果的有前途的工具。胃十二指肠切除术后胃排空延迟(DGE)仍然是成本和发病率的主要驱动力。
目的 确定RPD期间的技术变量是否与术后DGE相关。
设计,设置和参与者 从2008年10月3日至2016年9月27日,对在单个学术机构中进行的所有连续RPD的所有可用视频(n = 192)中进行的技术评估进行了回顾性研究。
曝光 RPD期间胃空肠吻合术的视频回顾。
主要结果和措施 根据国际胰腺外科研究小组的标准对延迟排空胃进行分类。视频分析回顾了胃空肠吻合术中具体的技术变量。使用多变量分析,将DGE与已知的患者变量和技术变量相关联,分别进行组合。
结果 在执行的410 RPD中,有192 RPD的视频(80名女性和112名男性;平均[SD]年龄为65.7 [11.1]岁)。胃排空延迟发生在41例患者中(21.4%; A级为15; B级为14; C级为12)。在多因素分析中对DGE起作用的患者变量为高龄(比值比[OR] 1.11; 95%CI,1.05-1.16;P <.001),胰管大小小(OR,0.84; 95%CI,0.72-0.98;P = .03)和术后假性动脉瘤(OR,17.29; 95%CI,2.34-127.78; P = .005)。但是,在多变量分析中导致DGE降低的技术变量包括胃与空肠假肢之间的流动角度(垂直30度以内)(OR,0.25; 95%CI,0.08-0.79;P = .02),更长的胃空肠吻合长度(OR,0.40; 95%CI,0.20-0.77;P = .006 ),以及机器人缝合的吻合(机器人缝合与吻合器缝合:OR,0.30; 95%CI, 0.09-0.95;P = 0.04)。
结论与相关性 这项研究通过回顾手术时获得的视频,检查了可修改的技术因素,并提出了在RPD期间通过手术建造胃空肠吻合术可以减少DGE发生率的方法,以此作为改善预期质量的框架。


























 京公网安备 11010802027423号
京公网安备 11010802027423号