当前位置:
X-MOL 学术
›
JAMA Intern. Med.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Effect of Protein Intake on Lean Body Mass in Functionally Limited Older Men
JAMA Internal Medicine ( IF 22.5 ) Pub Date : 2018-04-01 , DOI: 10.1001/jamainternmed.2018.0008 Shalender Bhasin 1 , Caroline M Apovian 2 , Thomas G Travison 3, 4 , Karol Pencina 1 , Lynn L Moore 5 , Grace Huang 1 , Wayne W Campbell 6 , Zhuoying Li 1 , Andrew S Howland 1 , Ruo Chen 1 , Philip E Knapp 2 , Martha R Singer 5 , Mitali Shah 2 , Kristina Secinaro 1 , Richard V Eder 1 , Kathleen Hally 1 , Haley Schram 1 , Richelle Bearup 1 , Yusnie M Beleva 1 , Ashley C McCarthy 2 , Erin Woodbury 1 , Jennifer McKinnon 1 , Geeta Fleck 1 , Thomas W Storer 1 , Shehzad Basaria 1
JAMA Internal Medicine ( IF 22.5 ) Pub Date : 2018-04-01 , DOI: 10.1001/jamainternmed.2018.0008 Shalender Bhasin 1 , Caroline M Apovian 2 , Thomas G Travison 3, 4 , Karol Pencina 1 , Lynn L Moore 5 , Grace Huang 1 , Wayne W Campbell 6 , Zhuoying Li 1 , Andrew S Howland 1 , Ruo Chen 1 , Philip E Knapp 2 , Martha R Singer 5 , Mitali Shah 2 , Kristina Secinaro 1 , Richard V Eder 1 , Kathleen Hally 1 , Haley Schram 1 , Richelle Bearup 1 , Yusnie M Beleva 1 , Ashley C McCarthy 2 , Erin Woodbury 1 , Jennifer McKinnon 1 , Geeta Fleck 1 , Thomas W Storer 1 , Shehzad Basaria 1
Affiliation
|
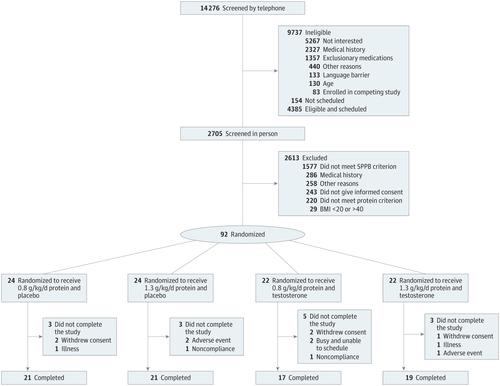
Importance The Institute of Medicine set the recommended dietary allowance (RDA) for protein at 0.8 g/kg/d for the entire adult population. It remains controversial whether protein intake greater than the RDA is needed to maintain protein anabolism in older adults. Objective To investigate whether increasing protein intake to 1.3 g/kg/d in older adults with physical function limitations and usual protein intake within the RDA improves lean body mass (LBM), muscle performance, physical function, fatigue, and well-being and augments LBM response to a muscle anabolic drug. Design, Setting, and Participants This randomized clinical trial with a 2 × 2 factorial design was conducted in a research center. A modified intent-to-treat analytic strategy was used. Participants were 92 functionally limited men 65 years or older with usual protein intake less thanor equal to 0.83 g/kg/d within the RDA. The first participant was randomized on September 21, 2011, and the last participant completed the study on January 19, 2017. Interventions Participants were randomized for 6 months to controlled diets with 0.8 g/kg/d of protein plus placebo, 1.3 g/kg/d of protein plus placebo, 0.8 g/kg/d of protein plus testosterone enanthate (100 mg weekly), or 1.3 g/kg/d of protein plus testosterone. Prespecified energy and protein contents were provided through custom-prepared meals and supplements. Main Outcomes and Measures The primary outcome was change in LBM. Secondary outcomes were muscle strength, power, physical function, health-related quality of life, fatigue, affect balance, and well-being. Results Among 92 men (mean [SD] age, 73.0 [5.8] years), the 4 study groups did not differ in baseline characteristics. Changes from baseline in LBM (0.31 kg; 95% CI, −0.46 to 1.08 kg; P = .43) and appendicular (0.04 kg; 95% CI, −0.48 to 0.55 kg; P = .89) and trunk (0.24 kg; 95% CI, −0.17 to 0.66 kg; P = .24) lean mass, as well as muscle strength and power, walking speed and stair-climbing power, health-related quality of life, fatigue, and well-being, did not differ between men assigned to 0.8 vs 1.3 g/kg/d of protein regardless of whether they received testosterone or placebo. Fat mass decreased in participants given higher protein but did not change in those given the RDA: between-group differences were significant (difference, −1.12 kg; 95% CI, −2.04 to −0.21; P = .02). Conclusions and Relevance Protein intake exceeding the RDA did not increase LBM, muscle performance, physical function, or well-being measures or augment anabolic response to testosterone in older men with physical function limitations whose usual protein intakes were within the RDA. The RDA for protein is sufficient to maintain LBM, and protein intake exceeding the RDA does not promote LBM accretion or augment anabolic response to testosterone. Trial Registration clinicaltrials.gov Identifier: NCT01275365
中文翻译:

蛋白质摄入量对功能受限的老年男性去脂体重的影响
重要性 医学研究所将所有成年人口的蛋白质推荐膳食摄入量 (RDA) 定为 0.8 克/公斤/天。老年人的蛋白质合成代谢是否需要高于每日推荐摄入量(RDA),仍存在争议。目的 研究将身体功能受限的老年人的蛋白质摄入量增加至 1.3 g/kg/d,并且将蛋白质摄入量控制在 RDA 范围内,是否可以改善去脂体重 (LBM)、肌肉性能、身体功能、疲劳和幸福感,并增强健康水平。 LBM 对肌肉合成代谢药物的反应。设计、设置和参与者 这项随机临床试验采用 2 × 2 析因设计,在研究中心进行。使用修改后的意向治疗分析策略。参与者是 92 名 65 岁或以上的功能受限男性,通常蛋白质摄入量低于或等于 RDA 内的 0.83 克/公斤/天。第一个参与者于 2011 年 9 月 21 日被随机分配,最后一个参与者于 2017 年 1 月 19 日完成研究。 干预措施 参与者被随机分配 6 个月,接受 0.8 g/kg/d 蛋白质加安慰剂、1.3 g/kg 的控制饮食。 /d 蛋白质加安慰剂,0.8 g/kg/d 蛋白质加庚酸睾酮(每周 100 mg),或 1.3 g/kg/d 蛋白质加睾酮。通过定制膳食和补充剂提供预先指定的能量和蛋白质含量。主要成果和措施 主要成果是 LBM 的变化。次要结果是肌肉力量、力量、身体功能、健康相关的生活质量、疲劳、情感平衡和幸福感。结果 在 92 名男性(平均 [SD] 年龄,73.0 [5.8] 岁)中,4 个研究组的基线特征没有差异。 LBM 相对于基线的变化(0.31 kg;95% CI,-0.46 至 1.08 kg;P = .43)和阑尾(0.04 kg;95% CI,-0.48至0.55 kg;P = .89)和躯干(0.24 kg;95% CI,-0.17至0.66 kg;P = .24)瘦体重,以及每天摄入 0.8 克/公斤蛋白质和 1.3 克/公斤/天蛋白质的男性之间的肌肉力量和力量、步行速度和爬楼梯力量、与健康相关的生活质量、疲劳和幸福感没有差异,无论他们是否接受睾丸激素或安慰剂。给予较高蛋白质的参与者脂肪量减少,但给予 RDA 的参与者脂肪量没有变化:组间差异显着(差异,-1.12 kg;95% CI,-2.04 至 -0.21;P = .02)。结论和相关性 对于身体功能受限且通常蛋白质摄入量在 RDA 范围内的老年男性来说,超过 RDA 的蛋白质摄入量不会增加 LBM、肌肉性能、身体功能或健康指标,也不会增强对睾酮的合成代谢反应。蛋白质的 RDA 足以维持 LBM,超过 RDA 的蛋白质摄入量不会促进 LBM 增加或增强对睾酮的合成代谢反应。试验注册临床试验。政府标识符:NCT01275365
更新日期:2018-04-01
中文翻译:
蛋白质摄入量对功能受限的老年男性去脂体重的影响
重要性 医学研究所将所有成年人口的蛋白质推荐膳食摄入量 (RDA) 定为 0.8 克/公斤/天。老年人的蛋白质合成代谢是否需要高于每日推荐摄入量(RDA),仍存在争议。目的 研究将身体功能受限的老年人的蛋白质摄入量增加至 1.3 g/kg/d,并且将蛋白质摄入量控制在 RDA 范围内,是否可以改善去脂体重 (LBM)、肌肉性能、身体功能、疲劳和幸福感,并增强健康水平。 LBM 对肌肉合成代谢药物的反应。设计、设置和参与者 这项随机临床试验采用 2 × 2 析因设计,在研究中心进行。使用修改后的意向治疗分析策略。参与者是 92 名 65 岁或以上的功能受限男性,通常蛋白质摄入量低于或等于 RDA 内的 0.83 克/公斤/天。第一个参与者于 2011 年 9 月 21 日被随机分配,最后一个参与者于 2017 年 1 月 19 日完成研究。 干预措施 参与者被随机分配 6 个月,接受 0.8 g/kg/d 蛋白质加安慰剂、1.3 g/kg 的控制饮食。 /d 蛋白质加安慰剂,0.8 g/kg/d 蛋白质加庚酸睾酮(每周 100 mg),或 1.3 g/kg/d 蛋白质加睾酮。通过定制膳食和补充剂提供预先指定的能量和蛋白质含量。主要成果和措施 主要成果是 LBM 的变化。次要结果是肌肉力量、力量、身体功能、健康相关的生活质量、疲劳、情感平衡和幸福感。结果 在 92 名男性(平均 [SD] 年龄,73.0 [5.8] 岁)中,4 个研究组的基线特征没有差异。 LBM 相对于基线的变化(0.31 kg;95% CI,-0.46 至 1.08 kg;P = .43)和阑尾(0.04 kg;95% CI,-0.48至0.55 kg;P = .89)和躯干(0.24 kg;95% CI,-0.17至0.66 kg;P = .24)瘦体重,以及每天摄入 0.8 克/公斤蛋白质和 1.3 克/公斤/天蛋白质的男性之间的肌肉力量和力量、步行速度和爬楼梯力量、与健康相关的生活质量、疲劳和幸福感没有差异,无论他们是否接受睾丸激素或安慰剂。给予较高蛋白质的参与者脂肪量减少,但给予 RDA 的参与者脂肪量没有变化:组间差异显着(差异,-1.12 kg;95% CI,-2.04 至 -0.21;P = .02)。结论和相关性 对于身体功能受限且通常蛋白质摄入量在 RDA 范围内的老年男性来说,超过 RDA 的蛋白质摄入量不会增加 LBM、肌肉性能、身体功能或健康指标,也不会增强对睾酮的合成代谢反应。蛋白质的 RDA 足以维持 LBM,超过 RDA 的蛋白质摄入量不会促进 LBM 增加或增强对睾酮的合成代谢反应。试验注册临床试验。政府标识符:NCT01275365










































 京公网安备 11010802027423号
京公网安备 11010802027423号