Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Effect of a Low-Intensity PSA-Based Screening Intervention on Prostate Cancer Mortality
JAMA ( IF 63.1 ) Pub Date : 2018-03-06 , DOI: 10.1001/jama.2018.0154 Richard M Martin 1, 2 , Jenny L Donovan 1, 3 , Emma L Turner 1 , Chris Metcalfe 1, 4 , Grace J Young 1, 4 , Eleanor I Walsh 1 , J Athene Lane 1, 4 , Sian Noble 1 , Steven E Oliver 5 , Simon Evans 6 , Jonathan A C Sterne 1, 2 , Peter Holding 7 , Yoav Ben-Shlomo 1, 3 , Peter Brindle 8 , Naomi J Williams 1 , Elizabeth M Hill 1 , Siaw Yein Ng 1 , Jessica Toole 1 , Marta K Tazewell 1 , Laura J Hughes 9 , Charlotte F Davies 1 , Joanna C Thorn 1 , Elizabeth Down 1 , George Davey Smith 1, 10 , David E Neal 7, 9 , Freddie C Hamdy 7 ,
JAMA ( IF 63.1 ) Pub Date : 2018-03-06 , DOI: 10.1001/jama.2018.0154 Richard M Martin 1, 2 , Jenny L Donovan 1, 3 , Emma L Turner 1 , Chris Metcalfe 1, 4 , Grace J Young 1, 4 , Eleanor I Walsh 1 , J Athene Lane 1, 4 , Sian Noble 1 , Steven E Oliver 5 , Simon Evans 6 , Jonathan A C Sterne 1, 2 , Peter Holding 7 , Yoav Ben-Shlomo 1, 3 , Peter Brindle 8 , Naomi J Williams 1 , Elizabeth M Hill 1 , Siaw Yein Ng 1 , Jessica Toole 1 , Marta K Tazewell 1 , Laura J Hughes 9 , Charlotte F Davies 1 , Joanna C Thorn 1 , Elizabeth Down 1 , George Davey Smith 1, 10 , David E Neal 7, 9 , Freddie C Hamdy 7 ,
Affiliation
|
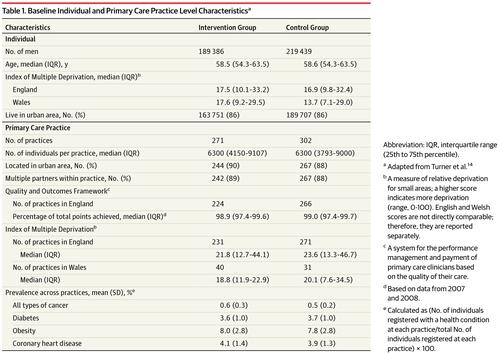
Importance Prostate cancer screening remains controversial because potential mortality or quality-of-life benefits may be outweighed by harms from overdetection and overtreatment. Objective To evaluate the effect of a single prostate-specific antigen (PSA) screening intervention and standardized diagnostic pathway on prostate cancer–specific mortality. Design, Setting, and Participants The Cluster Randomized Trial of PSA Testing for Prostate Cancer (CAP) included 419 582 men aged 50 to 69 years and was conducted at 573 primary care practices across the United Kingdom. Randomization and recruitment of the practices occurred between 2001 and 2009; patient follow-up ended on March 31, 2016. Intervention An invitation to attend a PSA testing clinic and receive a single PSA test vs standard (unscreened) practice. Main Outcomes and Measures Primary outcome: prostate cancer–specific mortality at a median follow-up of 10 years. Prespecified secondary outcomes: diagnostic cancer stage and Gleason grade (range, 2-10; higher scores indicate a poorer prognosis) of prostate cancers identified, all-cause mortality, and an instrumental variable analysis estimating the causal effect of attending the PSA screening clinic. Results Among 415 357 randomized men (mean [SD] age, 59.0 [5.6] years), 189 386 in the intervention group and 219 439 in the control group were included in the analysis (n = 408 825; 98%). In the intervention group, 75 707 (40%) attended the PSA testing clinic and 67 313 (36%) underwent PSA testing. Of 64 436 with a valid PSA test result, 6857 (11%) had a PSA level between 3 ng/mL and 19.9 ng/mL, of whom 5850 (85%) had a prostate biopsy. After a median follow-up of 10 years, 549 (0.30 per 1000 person-years) died of prostate cancer in the intervention group vs 647 (0.31 per 1000 person-years) in the control group (rate difference, −0.013 per 1000 person-years [95% CI, −0.047 to 0.022]; rate ratio [RR], 0.96 [95% CI, 0.85 to 1.08]; P = .50). The number diagnosed with prostate cancer was higher in the intervention group (n = 8054; 4.3%) than in the control group (n = 7853; 3.6%) (RR, 1.19 [95% CI, 1.14 to 1.25]; P < .001). More prostate cancer tumors with a Gleason grade of 6 or lower were identified in the intervention group (n = 3263/189 386 [1.7%]) than in the control group (n = 2440/219 439 [1.1%]) (difference per 1000 men, 6.11 [95% CI, 5.38 to 6.84]; P < .001). In the analysis of all-cause mortality, there were 25 459 deaths in the intervention group vs 28 306 deaths in the control group (RR, 0.99 [95% CI, 0.94 to 1.03]; P = .49). In the instrumental variable analysis for prostate cancer mortality, the adherence-adjusted causal RR was 0.93 (95% CI, 0.67 to 1.29; P = .66). Conclusions and Relevance Among practices randomized to a single PSA screening intervention vs standard practice without screening, there was no significant difference in prostate cancer mortality after a median follow-up of 10 years but the detection of low-risk prostate cancer cases increased. Although longer-term follow-up is under way, the findings do not support single PSA testing for population-based screening. Trial Registration ISRCTN Identifier: ISRCTN92187251
中文翻译:

基于 PSA 的低强度筛查干预对前列腺癌死亡率的影响
前列腺癌筛查的重要性仍然存在争议,因为过度检测和过度治疗带来的危害可能会超过潜在的死亡率或生活质量益处。目的 评估单一前列腺特异性抗原(PSA)筛查干预和标准化诊断路径对前列腺癌特异性死亡率的影响。设计、设置和参与者前列腺癌 PSA 检测 (CAP) 的整群随机试验包括 419 582 名年龄 50 至 69 岁的男性,并在英国 573 个初级保健机构进行。 2001 年至 2009 年期间进行了随机化和招募;患者随访于 2016 年 3 月 31 日结束。 干预 邀请参加 PSA 测试诊所并接受单次 PSA 测试与标准(未经筛选)实践。主要结果和措施 主要结果:中位随访 10 年时前列腺癌特异性死亡率。预先指定的次要结果:确定的前列腺癌的诊断癌症分期和格里森分级(范围,2-10;分数越高表明预后越差)、全因死亡率以及估计参加 PSA 筛查诊所因果效应的工具变量分析。结果 在 415 357 名随机男性(平均 [SD] 年龄,59.0 [5.6] 岁)中,干预组 189 386 名,对照组 219 439 名被纳入分析(n = 408 825;98%)。在干预组中,75 707 人(40%)参加了 PSA 检测门诊,67 313 人(36%)接受了 PSA 检测。在 64 436 名具有有效 PSA 测试结果的人中,6857 名 (11%) 的 PSA 水平在 3 ng/mL 至 19.9 ng/mL 之间,其中 5850 名 (85%) 进行了前列腺活检。中位随访 10 年后,干预组有 549 人(每 1000 人年 0.30 人)死于前列腺癌,而干预组中有 647 人(每 1000 人年 0.30 人)死于前列腺癌。对照组每 1000 人年 31 例(比率差异,每 1000 人年 -0.013 [95% CI,-0.047 至 0.022];比率 [RR],0.96 [95% CI,0.85 至 1.08]; P = .50)。干预组诊断出前列腺癌的人数 (n = 8054; 4.3%) 高于对照组 (n = 7853; 3.6%) (RR, 1.19 [95% CI, 1.14 to 1.25]; P < . 001)。干预组 (n = 3263/189 386 [1.7%]) 中发现的格里森分级为 6 级或更低的前列腺癌肿瘤多于对照组 (n = 2440/219 439 [1.1%])(每组之间的差异) 1000 名男性,6.11 [95% CI,5.38 至 6.84];P < .001)。在全因死亡率分析中,干预组有 25 459 例死亡,对照组有 28 306 例死亡(RR,0.99 [95% CI,0.94 至 1.03];P = .49)。在前列腺癌死亡率的工具变量分析中,依从性调整后的因果 RR 为 0.93(95% CI,0.67 至 1.29;P = 0.66)。结论和相关性 在随机接受单一 PSA 筛查干预的实践与不进行筛查的标准实践之间,中位随访 10 年后,前列腺癌死亡率没有显着差异,但低风险前列腺癌病例的检出有所增加。尽管长期随访正在进行中,但研究结果并不支持单一 PSA 检测用于人群筛查。试用注册 ISRCTN 标识符:ISRCTN92187251
更新日期:2018-03-06
中文翻译:
基于 PSA 的低强度筛查干预对前列腺癌死亡率的影响
前列腺癌筛查的重要性仍然存在争议,因为过度检测和过度治疗带来的危害可能会超过潜在的死亡率或生活质量益处。目的 评估单一前列腺特异性抗原(PSA)筛查干预和标准化诊断路径对前列腺癌特异性死亡率的影响。设计、设置和参与者前列腺癌 PSA 检测 (CAP) 的整群随机试验包括 419 582 名年龄 50 至 69 岁的男性,并在英国 573 个初级保健机构进行。 2001 年至 2009 年期间进行了随机化和招募;患者随访于 2016 年 3 月 31 日结束。 干预 邀请参加 PSA 测试诊所并接受单次 PSA 测试与标准(未经筛选)实践。主要结果和措施 主要结果:中位随访 10 年时前列腺癌特异性死亡率。预先指定的次要结果:确定的前列腺癌的诊断癌症分期和格里森分级(范围,2-10;分数越高表明预后越差)、全因死亡率以及估计参加 PSA 筛查诊所因果效应的工具变量分析。结果 在 415 357 名随机男性(平均 [SD] 年龄,59.0 [5.6] 岁)中,干预组 189 386 名,对照组 219 439 名被纳入分析(n = 408 825;98%)。在干预组中,75 707 人(40%)参加了 PSA 检测门诊,67 313 人(36%)接受了 PSA 检测。在 64 436 名具有有效 PSA 测试结果的人中,6857 名 (11%) 的 PSA 水平在 3 ng/mL 至 19.9 ng/mL 之间,其中 5850 名 (85%) 进行了前列腺活检。中位随访 10 年后,干预组有 549 人(每 1000 人年 0.30 人)死于前列腺癌,而干预组中有 647 人(每 1000 人年 0.30 人)死于前列腺癌。对照组每 1000 人年 31 例(比率差异,每 1000 人年 -0.013 [95% CI,-0.047 至 0.022];比率 [RR],0.96 [95% CI,0.85 至 1.08]; P = .50)。干预组诊断出前列腺癌的人数 (n = 8054; 4.3%) 高于对照组 (n = 7853; 3.6%) (RR, 1.19 [95% CI, 1.14 to 1.25]; P < . 001)。干预组 (n = 3263/189 386 [1.7%]) 中发现的格里森分级为 6 级或更低的前列腺癌肿瘤多于对照组 (n = 2440/219 439 [1.1%])(每组之间的差异) 1000 名男性,6.11 [95% CI,5.38 至 6.84];P < .001)。在全因死亡率分析中,干预组有 25 459 例死亡,对照组有 28 306 例死亡(RR,0.99 [95% CI,0.94 至 1.03];P = .49)。在前列腺癌死亡率的工具变量分析中,依从性调整后的因果 RR 为 0.93(95% CI,0.67 至 1.29;P = 0.66)。结论和相关性 在随机接受单一 PSA 筛查干预的实践与不进行筛查的标准实践之间,中位随访 10 年后,前列腺癌死亡率没有显着差异,但低风险前列腺癌病例的检出有所增加。尽管长期随访正在进行中,但研究结果并不支持单一 PSA 检测用于人群筛查。试用注册 ISRCTN 标识符:ISRCTN92187251










































 京公网安备 11010802027423号
京公网安备 11010802027423号