JAMA Surgery ( IF 15.7 ) Pub Date : 2018-02-01 , DOI: 10.1001/jamasurg.2017.3799 Jasmine A Khubchandani 1 , Angela M Ingraham 2 , Vijaya T Daniel 3 , Didem Ayturk 3 , Catarina I Kiefe 4 , Heena P Santry 3, 4
|
Importance Owing to lack of adequate emergency care infrastructure and decline in general surgery workforce, the United States faces a crisis in access to emergency general surgery (EGS) care. Acute care surgery (ACS), an organized system of trauma, general surgery, and critical care, is a proposed solution; however, ACS diffusion remains poorly understood.
Objective To investigate geographic diffusion of ACS models of care and characterize the communities in which ACS implementation is lagging.
Design, Setting, and Participants A national survey on EGS practices was developed, tested, and administered at all 2811 US acute care hospitals providing EGS to adults between August 2015 and October 2015. Surgeons responsible for EGS coverage at these hospitals were approached. If these surgeons failed to respond to the initial survey implementation, secondary surgeons or chief medical officers at hospitals with only 1 general surgeon were approached.
Interventions Survey responses on ACS implementation were linked with geocoded hospital data and national census data to determine geographic diffusion of and access to ACS.
Main Outcomes and Measures We measured the distribution of hospitals with ACS models of care vs those without over time (diffusion) and by US counties characterized by sociodemographic characteristics of county residents (access).
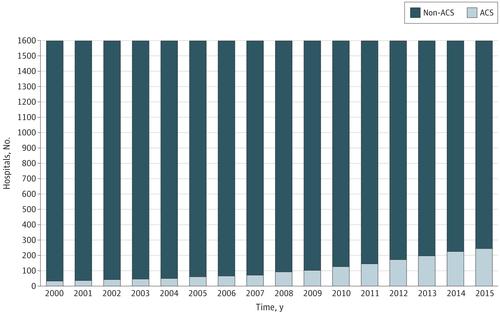
Results Survey response rate was 60% (n = 1690); 272 responding hospitals had implemented ACS by 2015, steadily increasing from 34 in 2001 to 125 in 2010. Acute care surgery implementation has not been uniform. Rural regions have limited ACS access, with hospitals in counties with greater than the 75th percentile population having 5.4 times higher odds (95% CI, 1.66-7.35) of implementing ACS than hospitals in counties with less than 25th percentile population. Communities with greater percentages of adults without a college degree also have limited ACS access (OR, 3.43; 95% CI, 1.81-6.48). However, incorporating EGS into ACS models may be a potential equalizer for poor, black, and Hispanic communities.
Conclusions and Relevance Understanding and addressing gaps in ACS implementation across communities will be crucial to ensuring health equity for US residents experiencing general surgery emergencies.
中文翻译:
急症护理手术的地理扩散和实施国家紧急普通外科危机的解决方案不平衡
重要性 由于缺乏足够的急诊基础设施和普外科劳动力的减少,美国面临着获得急诊普外科 (EGS) 护理的危机。急性护理手术(ACS)是一个由创伤、普通外科和重症监护组成的有组织的系统,是一个拟议的解决方案;然而,对于 ACS 扩散仍知之甚少。
目的 调查 ACS 护理模式的地理分布,并描述 ACS 实施滞后的社区特征。
设计、设置和参与者 2015 年 8 月至 2015 年 10 月期间,在向成人提供 EGS 的所有 2811 家美国急症护理医院中制定、测试和实施了一项关于 EGS 实践的全国调查。我们联系了这些医院负责 EGS 覆盖的外科医生。如果这些外科医生未能对最初的调查实施做出回应,则会联系二级外科医生或只有一名普通外科医生的医院的首席医疗官。
干预 措施 将 ACS 实施的调查回复与地理编码的医院数据和国家人口普查数据联系起来,以确定 ACS 的地理扩散和获取。
主要成果和措施 我们测量了采用 ACS 护理模式的医院与未采用 ACS 护理模式的医院的分布情况(扩散),以及以县居民社会人口特征为特征的美国县(访问)。
结果 调查回复率为 60% (n = 1690);截至 2015 年,已有 272 家响应医院实施了 ACS,从 2001 年的 34 家稳步增加到 2010 年的 125 家。急症护理手术的实施情况并不统一。农村地区获得 ACS 的机会有限,人口超过 75% 的县的医院实施 ACS 的几率是人口低于 25% 的县的医院的 5.4 倍(95% CI,1.66-7.35)。没有大学学位的成年人比例较高的社区获得 ACS 的机会也有限(OR,3.43;95% CI,1.81-6.48)。然而,将 EGS 纳入 ACS 模型可能是贫困、黑人和西班牙裔社区的潜在均衡器。
结论和相关性 了解并解决跨社区 ACS 实施方面的差距对于确保经历普通外科紧急情况的美国居民的健康公平至关重要。










































 京公网安备 11010802027423号
京公网安备 11010802027423号