JAMA Surgery ( IF 15.7 ) Pub Date : 2018-02-01 , DOI: 10.1001/jamasurg.2017.3787 Charles A. Karcutskie 1 , Arjuna Dharmaraja 1 , Jaimin Patel 1 , Sarah A. Eidelson 1 , Anish B. Padiadpu 1 , Arch G. Martin 1 , Gabriel Lama 1 , Edward B. Lineen 1 , Nicholas Namias 1 , Carl I. Schulman 1 , Kenneth G. Proctor 1
|
Importance The efficacy of anti–factor Xa (anti-Xa)–guided dosing of thromboprophylaxis after trauma remains controversial.
Objective To assess whether dosing of enoxaparin sodium based on peak anti-Xa levels is associated with the venous thromboembolism (VTE) rate after trauma.
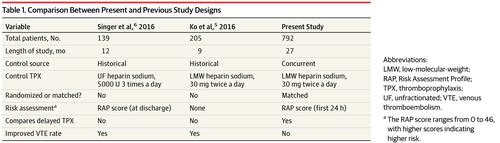
Design, Setting, and Participants Retrospective review of 950 consecutive adults admitted to a single level I trauma intensive care unit for more than 48 hours from December 1, 2014, through March 31, 2017. Within 24 hours of admission, these trauma patients were screened with the Greenfield Risk Assessment Profile (RAP) (possible score range, 0-46). Patients younger than 18 years and those with VTE on admission were excluded, resulting in a study population of 792 patients.
Exposures The control group received fixed doses of either heparin sodium, 5000 U 3 times a day, or enoxaparin sodium, 30 mg twice a day. The adjustment cohort initially received enoxaparin sodium, 30 mg twice a day. A peak anti-Xa level was drawn 4 hours after the third dose. If the anti-Xa level was 0.2 IU/mL or higher, no adjustment was made. If the anti-Xa level was less than 0.2 IU/mL, each dose was increased by 10 mg. The process was repeated up to a maximum dose of 60 mg twice a day.
Main Outcomes and Measures Rates of VTE were measured. Venous duplex ultrasonography and computed tomographic angiography were used for diagnosis.
Results The study population comprised 792 patients with a mean (SD) age of 46 (19) years and was composed of 598 men (75.5%). The control group comprised 570 patients, was older, and had a longer time to thromboprophylaxis initiation. The adjustment group consisted of 222 patients, was more severely injured, and had a longer hospital length of stay. The mean (SD) RAP scores were 9 (4) for the control group and 9 (5) for the adjustment group (P = .28). The VTE rates were similar for both groups (34 patients [6.0%] vs 15 [6.8%]; P = .68). Prophylactic anti-Xa levels were reached in 119 patients (53.6%) in the adjustment group. No difference in VTE rates was observed between those who became prophylactic and those who did not (7 patients [5.9%] vs 8 [7.8%]; P = .58). To control for confounders, 132 patients receiving standard fixed-dose enoxaparin were propensity matched to 84 patients receiving dose-adjusted enoxaparin. The VTE rates remained similar between the control and adjustment groups (3 patients [2.3%] vs 3 [3.6%]; P = .57).
Conclusions and Relevance Rates of VTE were not reduced with anti-Xa–guided dosing, and almost half of the patients never reached prophylactic anti-Xa levels; achieving those levels did not decrease VTE rates. Thus, other targets, such as platelets, may be necessary to optimize thromboprophylaxis after trauma.
中文翻译:
抗因子Xa指导的依诺肝素剂量与创伤后静脉血栓栓塞的关系
重要性 在创伤后,抗凝血因子Xa(anti-Xa)指导的血栓预防剂量仍然是有争议的。
目的 评估基于抗Xa峰值的依诺肝素钠剂量与创伤后静脉血栓栓塞(VTE)率是否相关。
设计,背景和参与者 自2014年12月1日至2017年3月31日,对连续950多个进入一级I创伤重症监护病房的连续成人进行回顾性回顾。入院24小时内,对这些创伤患者进行了筛查使用Greenfield风险评估配置文件(RAP)(可能的得分范围是0-46)。排除了18岁以下的患者和入院时接受VTE的患者,因此研究人群为792名患者。
暴露 对照组每天接受固定剂量的肝素钠(每天5000 U 3次)或依诺肝素钠(每天30 mg)两次。调整队列最初接受每天两次两次的30 mg依诺肝素钠。在第三次给药后4小时,获得了最高的抗Xa水平。如果抗Xa水平为0.2 IU / mL或更高,则不进行调整。如果抗Xa水平低于0.2 IU / mL,则每剂剂量应增加10 mg。每天两次,重复此过程直至最大剂量为60 mg。
主要结果和衡量指标 VTE的发生率。静脉双路超声检查和计算机断层血管造影用于诊断。
结果 研究人群包括792例患者,平均(SD)年龄为46(19)岁,由598名男性(75.5%)组成。对照组包括570名患者,年龄较大,并且有更长的时间进行血栓预防。调整组由222例患者组成,受伤更严重,住院时间更长。对照组的平均(SD)RAP评分为9(4),而调整组的RAP评分为9(5)(P = 0.28)。两组的VTE率相似(34例[6.0%]对15例[6.8%];P = 0.68)。调整组中有119例患者(53.6%)达到了预防性的Xa预防水平。预防组和未预防组之间的VTE率无差异(7例[5.9%]对8例[7.8%];P = .58)。为了控制混杂因素,将132例接受标准固定剂量依诺肝素的患者与84例接受剂量调整后的依诺肝素的患者相匹配。对照组和调整组之间的VTE率仍然相似(3例[2.3%] vs 3 [3.6%];P = 0.57)。
结论 抗Xa指导剂量并没有降低VTE的相关性和相关性,几乎一半的患者从未达到预防性的抗Xa水平。达到这些水平并不会降低VTE率。因此,可能需要其他目标(例如血小板)来优化创伤后的血栓预防。










































 京公网安备 11010802027423号
京公网安备 11010802027423号