JAMA Surgery ( IF 16.9 ) Pub Date : 2018-06-01 , DOI: 10.1001/jamasurg.2017.6117 Gurjit Sandhu 1 , Julie Thompson-Burdine 1 , Vahagn C. Nikolian 1 , Danielle C. Sutzko 1 , Kaustubh A. Prabhu 2 , Niki Matusko 1 , Rebecca M. Minter 3, 4
|
Importance A critical balance is sought between faculty supervision, appropriate resident autonomy, and patient safety in the operating room. Variability in the release of supervision during surgery represents a potential safety hazard to patients. A better understanding of intraoperative faculty-resident interactions is needed to determine what factors influence entrustment.
Objective To assess faculty and resident intraoperative entrustment behaviors and to determine whether faculty behaviors drive resident entrustability in the operating room.
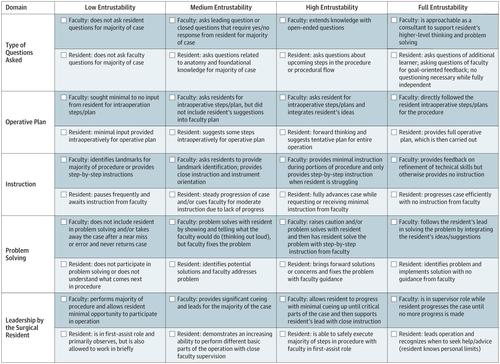
Design, Setting, and Participants This observational study was conducted from September 1, 2015, to August 31, 2016, at Michigan Medicine, the University of Michigan’s health care system. Two surgical residents, 1 medical student, 2 behavioral research scientists, and 1 surgical faculty member observed surgical intraoperative interactions between faculty and residents in 117 cases involving 28 faculty and 35 residents and rated entrustment behaviors. Without intervening in the interaction, 1 or 2 researchers observed each case and noted behaviors, verbal and nonverbal communication, and interaction processes. Immediately after the case, observers completed an assessment using OpTrust, a validated tool designed to assess progressive entrustment in the operating room. Purposeful sampling was used to generate variation in type of operation, case difficulty, faculty-resident pairings, faculty experience, and resident training level.
Main Outcomes and Measures Observer results in the form of entrustability scores (range, 1-4, with 4 indicating full entrustability) were compared with resident- and faculty-reported measures. Difficulty of operation was rated on a scale of 1 to 3 (higher scores indicate greater difficulty). Path analysis was used to explore direct and indirect effects of the predictors. Associations between resident entrustability and observation duration, observation month, and faculty entrustment scores were assessed by pairwise Pearson correlation coefficients.
Results Twenty-eight faculty and 35 residents were observed across 117 surgical cases from 4 surgical specialties. Cases observed by postgraduate year (PGY) of residents were distributed as follows: PGY-1, 21 (18%); 2, 15 (13%); 3, 17 (15%); 4, 27 (23%); 5, 28 (24%); and 6, 9 (8%). Case difficulty was evenly distributed: 36 (33%) were rated easy/straightforward; 43 (40%), moderately difficult; and 29 (27%), very difficult by attending physicians. Path analysis showed that the association of PGY with resident entrustability was mediated by faculty entrustment (0.23 [.03]; P < .001). At the univariate level, case difficulty (mean [SD] resident entrustability score range, 1.97 [0.75] for easy/straightforward cases to 2.59 [0.82] for very difficult cases; F = 6.69; P = .01), PGY (range, 1.31 [0.28] for PGY-1 to 3.16 [0.54] for PGY-6; F = 22.85; P < .001), and faculty entrustment (2.27 [0.79]; R2 = 0.91; P < .001) were significantly associated with resident entrustability. Mean (SD) resident entrustability scores were highest for very difficult cases (2.59 [0.82]) and PGY-6 (3.16 [0.54]).
Conclusions and Relevance Faculty entrustment behaviors may be the primary drivers of resident entrustability. Faculty entrustment is a feature of faculty surgeons’ teaching style and could be amenable to faculty development efforts.
中文翻译:
手术室教师与居民自治协会
重要性 在教师监督,适当的居民自治和手术室患者安全之间寻求关键的平衡。手术过程中监督释放的可变性对患者构成潜在的安全隐患。需要更好地了解术中教职工与住院医生之间的相互作用,以确定哪些因素会影响委托。
目的 评估教师和住院医生在术中的委托行为,并确定教师行为是否在手术室中驱动居民的委托能力。
设计,设置和参与者 这项观察性研究于2015年9月1日至2016年8月31日在密歇根大学的卫生保健系统密歇根医学中心进行。2名外科住院医师,1名医学生,2名行为研究科学家和1名外科教职员工在117例病例中观察了教职工与住院医师之间的外科术中互动,涉及28名教职工和35名住院医师,并评价了委托行为。在不干预互动的情况下,有1或2位研究人员观察了每种情况,并记录了行为,言语和非语言交流以及互动过程。案发后,观察员立即使用OpTrust(一种经过验证的工具,旨在评估手术室中的逐步委托)完成评估。使用有目的的抽样来产生操作类型,案例难度,教职员工对,
主要成果和措施 将以可信赖度评分(范围1-4,其中4表示完全可信赖)的形式观察者的结果与居民和教职员工报告的措施进行比较。手术难度等级为1到3(分数越高表示难度越大)。路径分析用于探索预测变量的直接和间接影响。通过成对的皮尔逊相关系数评估居民可委托性与观察持续时间,观察月和教职委托分数之间的关联。
结果 在4个外科专业的117例外科病例中,观察到28名教职员工和35名住院医师。按研究生年份(PGY)观察的病例分布如下:PGY-1,21(18%);2,15(13%); 3,17(15%); 4,27(23%); 5,28(24%); 和6、9(8%)。案例难度平均分配:36个案例(33%)被评为“简单/直接”;43(40%),中等难度;29人(占27%),很难去看医生。路径分析表明,PGY与居民可委托性之间的关联是由教师委托来介导的(0.23 [.03];P <.001)。在单变量水平上,案例难度(居民可信赖度的平均[SD]范围):对于简单/简单案例,为1.97 [0.75];对于非常困难的案例,为2.59 [0.82];F = 6.69;P = .01),PGY(范围,PGY-1为1.31 [0.28]至PGY-6为3.16 [0.54];F = 22.85;P <.001)和教职委托(2.27 [0.79];R 2 = 0.91; P <.001)与居民的可信赖性显着相关。在非常困难的情况下(2.59 [0.82])和在PGY-6(3.16 [0.54])上,居民的平均(SD)得分最高。
结论和相关性 教师的委托行为可能是居民信任的主要驱动力。教师委托是外科医生教学风格的一个特征,可能适合教师的发展努力。


























 京公网安备 11010802027423号
京公网安备 11010802027423号