Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Association of the Affordable Care Act Dependent Coverage Provision With Prenatal Care Use and Birth Outcomes
JAMA ( IF 63.1 ) Pub Date : 2018-02-13 , DOI: 10.1001/jama.2018.0030 Jamie R. Daw 1 , Benjamin D. Sommers 2, 3
JAMA ( IF 63.1 ) Pub Date : 2018-02-13 , DOI: 10.1001/jama.2018.0030 Jamie R. Daw 1 , Benjamin D. Sommers 2, 3
Affiliation
|
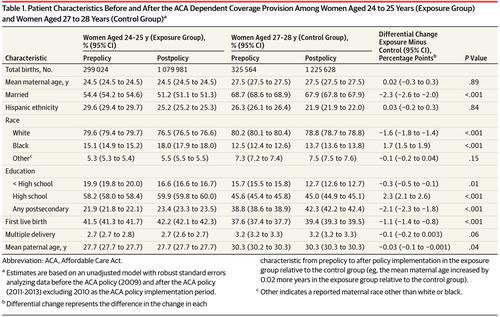
Importance The effect of the Affordable Care Act (ACA) dependent coverage provision on pregnancy-related health care and health outcomes is unknown. Objective To determine whether the dependent coverage provision was associated with changes in payment for birth, prenatal care, and birth outcomes. Design, Setting, and Participants Retrospective cohort study, using a differences-in-differences analysis of individual-level birth certificate data comparing live births among US women aged 24 to 25 years (exposure group) and women aged 27 to 28 years (control group) before (2009) and after (2011-2013) enactment of the dependent coverage provision. Results were stratified by marital status. Main Exposures The dependent coverage provision of the ACA, which allowed young adults to stay on their parent’s health insurance until age 26 years. Main Outcomes and Measures Primary outcomes were payment source for birth, early prenatal care (first visit in first trimester), and adequate prenatal care (a first trimester visit and 80% of expected visits). Secondary outcomes were cesarean delivery, premature birth, low birth weight, and infant neonatal intensive care unit (NICU) admission. Results The study population included 1 379 005 births among women aged 24-25 years (exposure group; 299 024 in 2009; 1 079 981 in 2011-2013), and 1 551 192 births among women aged 27-28 years (control group; 325 564 in 2009; 1 225 628 in 2011-2013). From 2011-2013, compared with 2009, private insurance payment for births increased in the exposure group (36.9% to 35.9% [difference, −1.0%]) compared with the control group (52.4% to 51.1% [difference, −1.3%]), adjusted difference-in-differences, 1.9 percentage points (95% CI, 1.6 to 2.1). Medicaid payment decreased in the exposure group (51.6% to 53.6% [difference, 2.0%]) compared with the control group (37.4% to 39.4% [difference, 1.9%]), adjusted difference-in-differences, −1.4 percentage points (95% CI, −1.7 to −1.2). Self-payment for births decreased in the exposure group (5.2% to 4.3% [difference, −0.9%]) compared with the control group (4.9% to 4.3% [difference, −0.5%]), adjusted difference-in-differences, −0.3 percentage points (95% CI, −0.4 to −0.1). Early prenatal care increased from 70% to 71.6% (difference, 1.6%) in the exposure group and from 75.7% to 76.8% (difference, 0.6%) in the control group (adjusted difference-in-differences, 0.6 percentage points [95% CI, 0.3 to 0.8]). Adequate prenatal care increased from 73.5% to 74.8% (difference, 1.3%) in the exposure group and from 77.5% to 78.8% (difference, 1.3%) in the control group (adjusted difference-in-differences, 0.4 percentage points [95% CI, 0.2 to 0.6]). Preterm birth decreased from 9.4% to 9.1% in the exposure group (difference, −0.3%) and from 9.1% to 8.9% in the control group (difference, −0.2%) (adjusted difference-in-differences, −0.2 percentage points (95% CI, −0.3 to −0.03). Overall, there were no significant changes in low birth weight, NICU admission, or cesarean delivery. In stratified analyses, changes in payment for birth, prenatal care, and preterm birth were concentrated among unmarried women. Conclusions and Relevance In this study of nearly 3 million births among women aged 24 to 25 years vs those aged 27 to 28 years, the Affordable Care Act dependent coverage provision was associated with increased private insurance payment for birth, increased use of prenatal care, and modest reduction in preterm births, but was not associated with changes in cesarean delivery rates, low birth weight, or NICU admission.
中文翻译:

平价医疗法案相关保险条款与产前护理使用和出生结果的关联
重要性 《平价医疗法案》(ACA) 依赖保险条款对妊娠相关医疗保健和健康结果的影响尚不清楚。目的 确定受抚养人保险条款是否与出生、产前护理和出生结果的支付变化有关。设计、设置和参与者 回顾性队列研究,使用个体水平出生证明数据的差异分析,比较 24 至 25 岁美国女性(暴露组)和 27 至 28 岁女性(对照组)的活产) 受抚养人保险条款颁布之前(2009 年)和之后(2011-2013 年)。结果按婚姻状况分层。主要风险 ACA 的受抚养人保险条款,允许年轻人继续使用父母的健康保险直到 26 岁。主要结果和措施 主要结果是出生的支付来源、早期产前护理(孕早期的首次访问)和充分的产前护理(孕早期访问和 80% 的预期访问)。次要结局是剖宫产、早产、低出生体重和婴儿新生儿重症监护病房 (NICU) 入院。结果 研究人群包括24-25岁女性生育1 379 005人(暴露组;2009年299 024人;2011-2013年1 079 981人),27-28岁女性生育1 551 192人(对照组; 2009 年为 325 564;2011-2013 年为 1 225 628)。2011-2013年,与2009年相比,暴露组(36.9%至35.9%[差异,-1.0%])与对照组(52.4%至51.1%[差异,-1.3%])的出生私人保险支付增加]),调整后的差异,1。9 个百分点(95% CI,1.6 到 2.1)。与对照组(37.4% 至 39.4% [差异,1.9%])相比,暴露组的医疗补助支付减少(51.6% 至 53.6% [差异,2.0%]),调整后差异,-1.4 个百分点(95% CI,-1.7 至 -1.2)。与对照组(4.9% 至 4.3% [差异,-0.5%])相比,暴露组(5.2% 至 4.3% [差异,-0.9%])的出生自费降低,调整后差异, -0.3 个百分点(95% CI,-0.4 至 -0.1)。暴露组的早期产前护理从 70% 增加到 71.6%(差异,1.6%),对照组从 75.7% 增加到 76.8%(差异,0.6%)(调整后的差异,0.6 个百分点 [95 % CI,0.3 至 0.8])。充分的产前护理从 73.5% 增加到 74.8%(差异,1. 3%) 在暴露组和从 77.5% 到 78.8%(差异,1.3%)在对照组(调整后的差异,0.4 个百分点 [95% CI,0.2 到 0.6])。暴露组的早产率从 9.4% 下降到 9.1%(差异,-0.3%),对照组从 9.1% 下降到 8.9%(差异,-0.2%)(调整后的差异,-0.2 个百分点) (95% CI,-0.3 至 -0.03)。总体而言,低出生体重、NICU 入住或剖宫产没有显着变化。在分层分析中,出生、产前护理和早产支付的变化集中在未婚女性。结论和相关性 在这项对 24 至 25 岁女性与 27 至 28 岁女性近 300 万次生育的研究中,
更新日期:2018-02-13
中文翻译:
平价医疗法案相关保险条款与产前护理使用和出生结果的关联
重要性 《平价医疗法案》(ACA) 依赖保险条款对妊娠相关医疗保健和健康结果的影响尚不清楚。目的 确定受抚养人保险条款是否与出生、产前护理和出生结果的支付变化有关。设计、设置和参与者 回顾性队列研究,使用个体水平出生证明数据的差异分析,比较 24 至 25 岁美国女性(暴露组)和 27 至 28 岁女性(对照组)的活产) 受抚养人保险条款颁布之前(2009 年)和之后(2011-2013 年)。结果按婚姻状况分层。主要风险 ACA 的受抚养人保险条款,允许年轻人继续使用父母的健康保险直到 26 岁。主要结果和措施 主要结果是出生的支付来源、早期产前护理(孕早期的首次访问)和充分的产前护理(孕早期访问和 80% 的预期访问)。次要结局是剖宫产、早产、低出生体重和婴儿新生儿重症监护病房 (NICU) 入院。结果 研究人群包括24-25岁女性生育1 379 005人(暴露组;2009年299 024人;2011-2013年1 079 981人),27-28岁女性生育1 551 192人(对照组; 2009 年为 325 564;2011-2013 年为 1 225 628)。2011-2013年,与2009年相比,暴露组(36.9%至35.9%[差异,-1.0%])与对照组(52.4%至51.1%[差异,-1.3%])的出生私人保险支付增加]),调整后的差异,1。9 个百分点(95% CI,1.6 到 2.1)。与对照组(37.4% 至 39.4% [差异,1.9%])相比,暴露组的医疗补助支付减少(51.6% 至 53.6% [差异,2.0%]),调整后差异,-1.4 个百分点(95% CI,-1.7 至 -1.2)。与对照组(4.9% 至 4.3% [差异,-0.5%])相比,暴露组(5.2% 至 4.3% [差异,-0.9%])的出生自费降低,调整后差异, -0.3 个百分点(95% CI,-0.4 至 -0.1)。暴露组的早期产前护理从 70% 增加到 71.6%(差异,1.6%),对照组从 75.7% 增加到 76.8%(差异,0.6%)(调整后的差异,0.6 个百分点 [95 % CI,0.3 至 0.8])。充分的产前护理从 73.5% 增加到 74.8%(差异,1. 3%) 在暴露组和从 77.5% 到 78.8%(差异,1.3%)在对照组(调整后的差异,0.4 个百分点 [95% CI,0.2 到 0.6])。暴露组的早产率从 9.4% 下降到 9.1%(差异,-0.3%),对照组从 9.1% 下降到 8.9%(差异,-0.2%)(调整后的差异,-0.2 个百分点) (95% CI,-0.3 至 -0.03)。总体而言,低出生体重、NICU 入住或剖宫产没有显着变化。在分层分析中,出生、产前护理和早产支付的变化集中在未婚女性。结论和相关性 在这项对 24 至 25 岁女性与 27 至 28 岁女性近 300 万次生育的研究中,










































 京公网安备 11010802027423号
京公网安备 11010802027423号